Download
1 / 45
460 likes | 645 Views
Maternal Diet for Lactation. Public Health Aspects of Lactation. Healthy People 2010. Who Breastfeeds? (Data source: Mothers’ Survey, Abbott Laboratories, Inc., Ross Products Division). Why do we care?. The Evidence for Breastfeeding- Pediatric Clinics of North America. February, 2001.

E N D
Who Breastfeeds? (Data source: Mothers’ Survey, Abbott Laboratories, Inc., Ross Products Division)
Why do we care? The Evidence for Breastfeeding- Pediatric Clinics of North America. February, 2001
Health Benefits for Infant • Lowered risk of infection: diarrhea, lower respiratory, otitis media, bacterial meningitis, botulism, UTI, Necrotizing enterocolitis • Lowered risk of sudden infant death syndrome • Possible lowered risk of IDDM, Crohn’s, ulcerative colitis, lymphoma • Probable enhanced cognitive development
Health Benefits for Mother • Possible reduction in hip fractures after menopause • Less postpartum bleeding • Reduced risk of premenopausal breast cancer
Economic Benefits for Families and Society • Direct - no formula to buy • Indirect - costs associated with infant illness - medical care and time lost from work
The Economic Benefits of Breastfeeding: A Review and Analysis. By JonWeimer. Food and Rural Economics Division, Economic Research Service,U.S. Department of Agriculture. Food Assistance and Nutrition ResearchReport No. 13., 2001
The resurgence of breastfeeding at the end of the second millennium. (Wright and Schanler, J Nutr. 131, 2001) • Between 1971 and 1995 increase was for all groups. • Between 1984 and 1995 increase was in groups less likely to breastfeed (low income, low education, African American, WIC) • Early resurgence of breastfeeding concurrent to “natural childbirth” and women’s movement in white well educated families
More recent increases associated with: • Increased knowledge of the benefits of breastfeeding by professionals (AAP 1997) • Successful breastfeeding interventions - especially in WIC • 47% of US infants on WIC • early 90s brought increased WIC & for breastfeeding promotion and increased maternal food package for BF
What can we do to improve breastfeeding rates? (Wright and Schanler, J Nutr. 131, 2001) • Social pressures that affect existing barriers that arise when the true costs of not breastfeeding are realized. • Workplace enhancements and more widespread coverage by the Family and Medical Leave Act. • Increased familiarity by medical providers
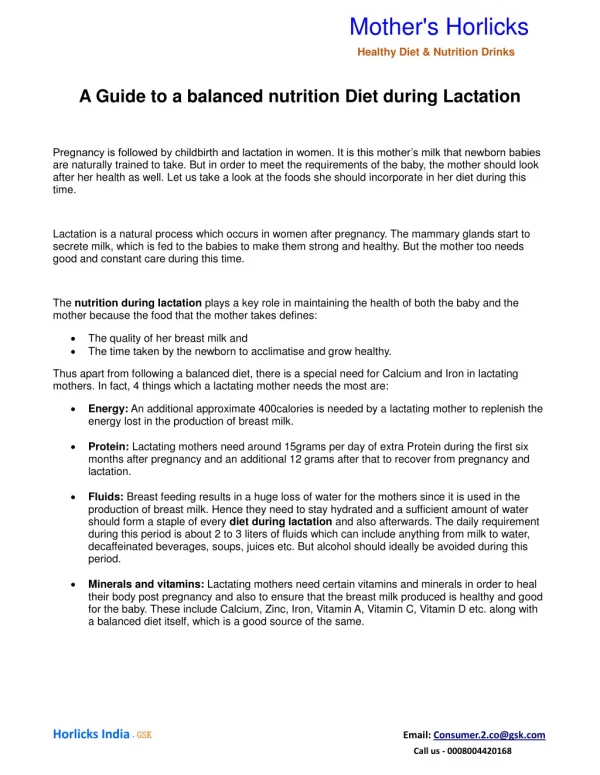
Basics • There is no one optimal set of rules for maternal diets • Women may choose not to breastfeed if the recommended dietary limitations and requirements are perceived as too difficult to follow
Basics “A balanced diet without excessive supplementation is the most physiologic and economic way to ensure good milk.” Ruth Lawrence, 1998
Basics IOM: Women are able to….“produce milk of sufficient quantity and quality to support growth and promote the health of infant - even when the mother’s supply of nutrients is limited.”
Maternal Diet and Milk Production • In extreme famine and malnutrition milk supply does eventually stop • In more moderate deprivation, like the Dutch famine, milk production decreased slightly, but was maintained at the expense of maternal tissue. • Effects of deficiencies may start at 1500 kcal/day
Energy • Wide variation between women & their infants • Dependent on maternal stores • 1989 RDA: 500 kcal/day over reference • Energy sparing adaptations • decreased BMR • decreased postprandial thermogenesis • decreased physical activity
Symposium: Maternal body composition, caloric restriction and exercise during lactation (Dewey, J Nutr, 1998) • For women with adequate stores, moderate weight loss does not adversely affect milk energy output. • Thin women will maintain milk energy output in the normal range as long as they are in neutral or positive energy balance. • It is only when thin women are in negative balance that milk energy output will be affected.
Maternal Energy Reserves > x 500 Milk energy output Kcal/day Maternal energy reserves < x 0 negative positive Maternal energy balance (kcal/day)
Symposium: Maternal body composition, caloric restriction and exercise during lactation (Dewey, J Nutr, 1998) • Protective factors when mothers are in negative energy balance: • a high level of aerobic exercise enhances body fat mobilization during lactation. • prolactin levels rise with exercise and negative energy balance leading to mobilization of fatty acids from adipose tissue or diet for milk synthesis (increased mammary lipoprotein lipase) • Frequency and intensity of infant sucking affect endocrine and autocrine regulation of milk synthesis.
Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance (McCrory, AJCN, 1999) • 3 groups of breastfeeding women ~12 weeks pp, on study for 11 days: • 35% energy deficit from diet alone (n=22) • 35% energy deficit from diet and exercise (n=22) • control group (n=23) • No significant difference in: • milk volume, composition, or energy output • infant weight
Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance (McCrory, AJCN, 1999)
Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance (McCrory, AJCN, 1999) • Interaction between group and baseline % body fat • diet only group: milk energy output increased in fatter women & decreased in leaner women • Plasma prolactin concentration was higher in energy deficit groups than the control group.
Protein • Protein content per volume is sufficient even in malnourished women • Supplementation of malnourished women increases total milk volume, but doesn’t increase % of kcal from protein
Cholesterol • Fat globule membrane includes cholesterol and phospholipids • Human milk has high levels of cholesterol; formula has none. • Proportions of cholesterol in human milk are not influenced by maternal diet.
Fatty Acids • Maternal diet has no effect on total % fat content of milk, but does influence kinds of fatty acids. • When mother is in energy balance, about 30% of fatty acids in milk comes from mother’s diet. • Mammary gland can synthesize n-9 fatty acids up to 16-C.
Essential fatty acid requirements of vegetarians in pregnancy, lactation, and infancy (Sanders, AJCN, 1999) • Many vegans and vegetarians have diets high in n-6 fatty acids and low in n-3 • ratios of 15:1 to 20:1 of linoleic to a-linolenic have been reported
Essential fatty acid requirements of vegetarians in pregnancy, lactation, and infancy (Sanders, AJCN, 1999)
Essential fatty acid requirements of vegetarians in pregnancy, lactation, and infancy (Sanders, AJCN, 1999) • Lower DHA levels have been observed in blood and artery phospholipids of infants of vegetarians. • Recommendations: • avoid excessive intakes of linoleic acid • recommended ratio of n-6 to n-3 is 4:1 to 10:1
Carbohydrate • Lactose concentration is very stable and is not affected by maternal diet
Water • “Forced” drinking is counter-productive • Illingworth and Kirkpatric (1953) reported that mothers produced less milk and babies gained less weight when they were forced to consume 107 oz per day compared to mothers with ad lib intakes averaging 69 oz per day.
Water “When fluids are restricted, mothers will experience a decrease in urine output, not in milk.” Lawrence, 1998
IOM Nutrient Recommendations • Examined US nutrient densities at 3 levels of energy intake: • 2700 (RDA for lactation) • 2200 (actual reported intakes) • 1800 (minimal level that should be considered on a restricted diet during lactation)
IOM Recommendations • Lactating women should be encouraged to obtain their nutrients from a well-balanced varied diet rather than from vitamin-mineral supplements. Specifically:
Eat a wide variety of breads and cereal grains, fruits, vegetables, milk products, and meats or meat alternates each day. • Take three or more servings of milk products daily. • Make a greater effort to eat vitamin A-rich vegetables or fruits often. • Be sure to drink when you are thirsty. You will need more fluid than usual. • If you drink coffee or other caffeinated beverages such as cola, do so in moderation. Two servings daily are unlikely to harm the infant. Caffeine passes into milk.
IOM Recommendations • There should be a well defined plan for the health care of the lactating woman that includes screening for nutritional problems and providing dietary guidance. • Women who plan to breastfeed or who are breastfeeding should be given realistic, health promoting advice about weight changes during lactation.
IOM Recommendations • Health care providers should be informed about the differences in growth between healthy breastfed and formula fed infants. • Steps should be taken to ensure adequate nutrition of all infants.