Download
1 / 66
770 likes | 1.59k Views
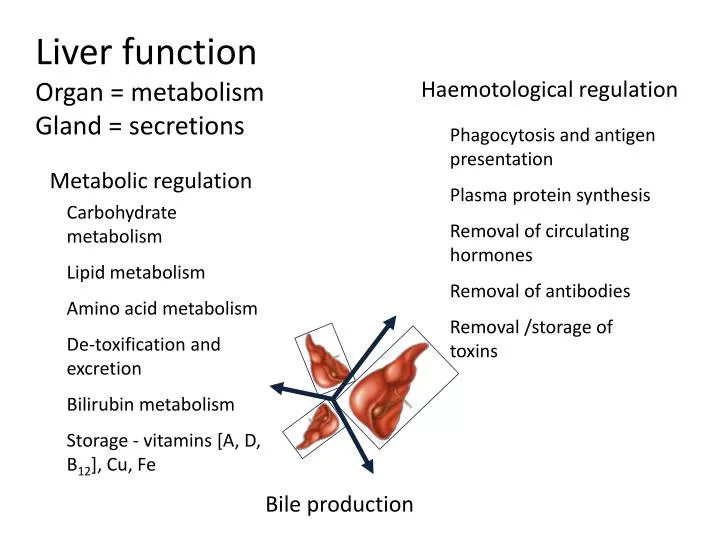
Metabolic regulation. Carbohydrate metabolism Lipid metabolism Amino acid metabolism De-toxification and excretion Bilirubin metabolism Storage - vitamins [A, D, B 12 ], Cu, Fe. Haemotological regulation. Phagocytosis and antigen presentation Plasma protein synthesis

E N D
Metabolic regulation Carbohydrate metabolism Lipid metabolism Amino acid metabolism De-toxification and excretion Bilirubin metabolism Storage - vitamins [A, D, B12], Cu, Fe Haemotological regulation Phagocytosis and antigen presentation Plasma protein synthesis Removal of circulating hormones Removal of antibodies Removal /storage of toxins Liver functionOrgan = metabolismGland = secretions Bile production
Carbohydrate metabolism Glycogenesis Glycogenolysis Gluconeogenesis IMPAIRMENT Hypoglycaemia Glucose Intolerance http://static.howstuffworks.com/gif/diabetes-glucose-regulation.gif
Lipid Metabolism • Lipoprotein synthesis • Oxidation of fats • Synthesis of cholesterol, phospholipids • Catabolism of steroids IMPAIRMENT Altered lipid profiles 2O Hyperaldosteronism →↑BP ↓K ↑pH 2O Hypercorticolism = Cushing’s disease Gonadal dysfunction → ∆ oestrogen:testestorone http://www.medscape.com/pi/editorial/clinupdates/2001/608/art-cu02.fig04.gif
Amino acid metabolism • Deamination and transamination of amino acids • Removal of ammonia • Synthesis of amino acids Hepatic encephalopathy Hypoproteinaemia IMPAIRMENT Source: seqcore.brcf.med.umich.edu/ mcb500/aametov.gif
Synthesis of hormones and plasma proteins……. • Insulin-like growth factor (IGF-1) → stimulated by pituitary growth hormone • Thrombopoietin → platelet production • Angiotensinogen (α-2-globulin) → hydrolysed by renin to angiotensin [renin-angiotensin-aldosterone system (RAAS)] • Heparin • Albumin • Extrinsic pathway clotting factors →I (fibrinogen), II (Prothrombin), IV, V, VI, and VII Clotting disorders, ↓ osmotic pressure IMPAIRMENT http://www.biosbcc.net/doohan/sample/images/blood%2520cells/clottingcascade
Bile production …. Water Bile Acids e.g. taurocholic and glycocholic acid Electrolytes Cholesterol Phospholipids Bilirubin IMPAIRMENT • Malabsorption of fats and fat soluble vitamins • Jaundice http://sbsweb.bangor.ac.uk/images/bsx1016/sm_liver_position
Detoxification – refer to Biochemistry and PK done in years 2/3. Phase I = modify Phase II = conjugate Reduced drug metabolism, reduced protein binding of drugs IMPAIRMENT http://www.aspartame-detox.info/images/brain-01.jpg
Filtration – Reticuloendothelial system Blood filtration, phagocytosis of bacteria and other particulate matter IMPAIRMENT Source :www.bu.edu/histology/ i/15204loa.jpg Exposure to bacteria and other particles
Symptoms of liver disease • Most symptoms non specific - anorexia, malaise, fatigue, fever • ↓ general health • cirrhotic habitus = wasted extremities plus protuberant abdomen with ascites • Generalised pruritus (itchiness) – due to retention of bile salts • Xanthelasma (fat build up under skin surface), xanthomas • Pale stools – lack of bile • Which of these is most specific? akimichi.homeunix.netXanthoma disappearance Document272 x 324 pixels - 55k - gif
Disorders of coagulation/circulation • ↑ bleeding and bruising • ↑ prothrombin time (PT) → extrinsic clotting pathway (Prothrombin ratio (PR) and international normalized ratio (INR) are derived measures of PT). • Thrombocytopaenia (↓platelets) • Dysfibrinogenaemia (altered fibrinogen function) • Portal hypertension → endothelial stretching and shear stress → ↑ NO → systemic vasodilation = hyperdynamic circulation • Hepatopulmonary syndrome = pulmonary vasodilation → ↑blood flow (ventilation-perfusion mismatch) → arterial desaturation • Cyanosis and clubbing → enlargement of distal fingers and toes. Due to vasodilation? http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18127.jpg
Liver disease? http://upload.wikimedia.org/wikipedia/en/thumb/e/e0/Gollum.PNG/220px-Gollum.PNG
Other changes • ↑ parotid salivary gland → fatty infiltation • Gynecomastia (mammary gland development in males), testicular atrophy, impotence • Amenorrhoea (absence of menstrual period) • Erythema (redness of skin) – build up of unmetabolised wastes in body http://www.sciencephoto.com/images/download_lo_res.html?id=771500153
Jaundice • Icterus (icteric) • Accumulation of bilirubin = hyperbilirubinaemia • Skin, conjuctiva, mucous membranes • Dark urine from renal excretion of bilirubin http://www.modulomedico.com/fotos/imgJaundiceBig.jpg
Serum chemistry/diagnostic testing • Breakdown product of haemoglobin • Globin = protein • Heme = iron containing → biliverdin (green bruising) → bilirubin → yellow (bruising/bile) • Bilirubin → conjugated with glucuronides in liver • Excreted in bile • Can be measured in the unconjugated (indirect) or conjugated (direct) form • Relatively insensitive indicator of liver disease Bilirubin Source:web.indstate.edu/thcme/ mwking/hemedegradation.jpg
From Swaminathan – Handbook of Clinical Biochemistry 2004 From Beckett - Lecture Notes : Clinical Biochemistry 7th ed 2005
Aminotransferases (ALT and AST) • Transaminase enzymes (aminotransferases) → reversible • transfer of an amino group between two a-keto acids. • Alanine aminotransferase = liver cytosol (ALT) • Aspartate aminotransferase = liver and other tissues (AST) • Reasonably sensitive indicators of liver disease, ALT >> AST Source: http://www.np.edu.sg/~dept-bio/biochemistry/aab/topics/asptrans.gif
Alterations in ALT and AST Mild elevations(<100U/L) • Fatty liver/non-alcoholic steatohepatitis (fatty degeneration) • Chronic viral hepatitis Moderate elevations(100-300 U/L) • Acute or chronic hepatitis • Alcoholic hepatitis • Mild/moderate inflammation High elevated(>300 U/L) • Acute viral hepatitis • Hepatic necrosis → drugs or toxins • Ischemic hepatitis /circulatory shock. VALUES CAN BE 500-1500 U/L • Values >3000 U/L- toxic necrosis, or severe hypoxia AST/ALT ratio • Significant overlap between different conditions BUT • > 2 suggestive alcoholic liver disease (if ALT < 500 U/L) • < 1 viral hepatitis can ↑ratio as fibrosis and cirrhosis develop
Alkaline phosphatases (ALP) • ALP = hydrolase →removes phosphate groups • Present in bile canaliculi, bone and placenta • ↑ sensitivity for hepatobiliary disease • ↓ specificity for hepatobiliary disease • Due to its numerous isoenzymes, its presence in non-hepatic tissues, and its sensitivity to drug induction
Increases in liver ALP • Cholestasis, cholecystitis, cholangitis, cirrhosis, hepatitis, fatty liver, liver tumour, liver metastases, drug intoxication • Drugs e.g. verapamil, carbamazepine, phenytoin, erythromycin, allopurinol, ranitidine • ↑ → enhanced synthesis rather than hepatocytic leakage • ↓ ≠ clinically significant • If source ↑ ALP is not clear check other liver enzymes
Gamma glutamyl transpeptidase (GGT) • GGT → hydrolysis of gamma-glutamyl peptide bonds • Biliary enzyme → obstruction of biliary tract + damage to biliary capillaries • Easily induced (alcohol, drugs) → disproportionately ↑ in alcoholic liver disease • Can be elevated in other diseases e.g. CHD, MI, COPD, pancreatitis, renal disease
Patterns of enzyme alterations Ramachandran and Kakar J Clin Pathol 2009;62;481-492 Histological patterns in drug-induced liver disease
ERCP = Endoscopic Retrograde Cholangiopancreatography From Beckett - Lecture Notes : Clinical Biochemistry 7th ed 2005
From Beckett - Lecture Notes : Clinical Biochemistry 7th ed 2005
Other tests • Haematology (anaemia, RBC parameters) • Clotting tests (PT) NOTE – these are vitamin K-dependent clotting factors • Lipid tests (total cholesterol, HDL, LDL, triglycerides) • Biochemistry (albumin, glucose) • Serology -Hepatitis virus -Antimitochondrial antibody (present in >90% of biliary cirrhosis cases) -Antinuclear factor- inflammatory marker -Antismooth muscle antibody-inflammatory marker -Alpha fetoprotein-hepatic carcinoma marker • Functional tests -Clearance tests (caffeine, bromosulphthalein), Elimination tests (galactose) • Imaging procedures -Abdominal radiographs -US, NMR, CT -Direct biliary visualisation → contrast studies • Liver Biopsy -Percutaneous -Surgical
Drug Induced Liver Disease (DILD) • > 1000 drugs → DILD • ↑Hz drug withdrawal from the market R x Reference Hughes et al. Use of laboratory test data: a process guide and reference for health care professionals. 2nd Ed, PSA, 2009.
Drug Induced Liver Disease (DILD) • Consider wherever altered liver function tests • However • Broad range of drugs • Wide variation in hepatic injury caused
Drug Induced Liver Disease (DILD) • Types of hepatic injury • Hepatitis • Cholestasis • Mixed • Fibrosis • Granulomatous lesions • Neoplasms http://www.health-writings.com/img/mk/drug-induced-liver-disease/drugs_MIC062ML.jpg
Drug induced hepatic failure http://www.path.cam.ac.uk/Normal/AR_Alimentary/LV_Liver/N_AR_LV_02.jpg http://mayoresearch.mayo.edu/mayo/research/nyberg_lab/images/histology.jpg
Drug Induced Liver Disease (DILD) • Other changes (functional) • Enzyme induction and inhibition • Dietary /other deficiencies e.g. cysteine, Vit K • Steatosis = fatty change • Phospholipidosis
Drug Induced Liver Disease (DILD) • Intrinsic • Dose related • Occurs within few days of use • Related to drug or toxic metabolite of drug • Known/reported/expected • Idiosyncratic • Unexpected • Variable latency • Not usually dose related
Factors affecting DILD • Age • Gender • Genetic factors • Nutritional status • Renal function • Dose and duration • Alcohol • Cigarette smoking • Other conditions- Hep C, HIV, RA
Paracetamol toxicity • Paracetamol = #1 drug → calls to poisons information centres in Australia and NZ. 1 • Paracetamol = #1 drug overdose → hospital presentation and admission. 2,3 • Hepatic failure and death → uncommon outcomes • #1 cause of acute fulminant hepatic failure in Western countries.4 Buckley N, Eddleston M. Paracetamol (acetaminophen) poisoning. Clin Evid 2005; (14): 1738-1744. Dart RC, Erdman AR, Olson KR, et al. Acetaminophen poisoning: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila) 2006; 44: 1-18. Linden CH, Rumack BH. Acetaminophen overdose. Emerg Med Clin North Am 1984; 2: 103-119. Ostapowicz G, Fontana RJ, Schiødt FV, et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med 2002; 137: 947-954.
Phases of paracetamol hepatotoxicity • PHASE 3 (72-96 H) • Centrilobular hepatic necrosis with continued abdominal pain • Jaundice • Coagulopathy • Hepatic encephalopathy • Nausea and vomiting • Renal failure • Fatality • PHASE 4 (4 D TO 3 WK) • Complete resolution of symptoms • Complete resolution of organ failure • PHASE 1 (0-24 H) • Asymptomatic • Anorexia • Nausea or vomiting • Malaise • Subclinical rise in serum transaminases levels begins at about 12 hours postingestion • PHASE 2 (18-72 H) • Right upper quadrant abdominal pain, anorexia, nausea, vomiting • Continued rise in serum transaminases levels • Admitted to hospital
Paracetamol toxicity • Toxicity when GSH reserves overwhelmed by N-acetyl-p-benzoquinone imine (NAPQi) • ± gastric lavage and activated charcoal • Treatment → IV N-acetylcysteine http://drugdiscoveryopinion.com/images/paracetamol_metabolism.jpg
Management plan- dose thresholds for NAC treatment ≠ serum readings <4 hours of poisoning Frank F S Daly, John S Fountain, Lindsay Murray, Andis Graudins and Nicholas ABuckley(2008).Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. MJA 2008; 188 (5): 296-302.
Management Plan Source- Frank F S Daly, John S Fountain, Lindsay Murray, Andis Graudins and Nicholas ABuckley(2008).Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. MJA 2008; 188 (5): 296-302. Source: Frank F S Daly, John S Fountain, Lindsay Murray, Andis Graudins and Nicholas A Buckley(2008).Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. MJA 2008; 188 (5): 296-302.
Management Plan cont… Source- Frank F S Daly, John S Fountain, Lindsay Murray, Andis Graudins and Nicholas ABuckley(2008).Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. MJA 2008; 188 (5): 296-302. Source: Frank F S Daly, John S Fountain, Lindsay Murray, Andis Graudins and Nicholas A Buckley(2008).Guidelines for the management of paracetamol poisoning in Australia and New Zealand — explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. MJA 2008; 188 (5): 296-302.
Management Plan cont… • Monitoring of liver function • Post –discharge patient education • Referral to Psychologist if needed
Kava (Piper methysticum) • Kava = plant native to South Pacific Islands • Western society → herbal remedy anxiety • Kavalactones = active components -6 KL ~ 95% of the activity • Anxiolytic effect ~ benzodiazepines -few side effects -limited cognitive and motor impairment • Kava → hepatotoxicity e.g. hepatitis, cirrhosis, fulminant liver failure, death • Banned in many countries • Australia → voluntary recall 2002
Isolated Perfused Rat Liver (IPRL) PUMP • Perfusate • Kavalactone • 95% O2/5% CO2 • Taurocholic acid • Krebs-Henseleit (KH) buffer Inferior Vena Cava Hepatic Portal Vein 37°C
10 µg/mL Kavain for 2 hours is hepatotoxic in IPRL studies Light Microscopy Scanning Electron Microscopy Control Liver Following Kavain Treatment Fu (2008) World J Gastroenterology 14: 541-546
Membranes and electron dense structures Distorted cell nuclei Autophagosome Whirled ER surrounding mitochondrion
Advice for case studies • Common things occur commonly. • Uncommon things don’t. • When you have eliminated the impossible, whatever remains, however improbable, must be the truth. Sherlock Holmes - The Sign of the Four (1890)
Case Study #1 – history and signalment • 68 YO male retired labourer • Lethargy but no pain • BW ↓19kg in the last 3 months • Eating normally up to last 3 weeks • Dark urine and pale stools • ‘Moderate’ drinker throughout lifetime
Clinical findings • Jaundice • Weakness • Palpable, non-tender mass in upper RHS abdominal quadrant
Serum chemistry • Bilirubin predominantly conjugated • ↑↑ ALP and GGT • Predominantly cholestasis • Pancreatic tumour obstructing common bile duct
Case Study #2 – history and signalment • 21 YO female student • Flu-like symptoms for 2 days • Condition deteriorating – dark urine, vomiting • Recently returned from long holiday in Asia