Download
1 / 90
1.02k likes | 2.5k Views
DISEASES OF THYROID GLAND 1. By PROFESSOR MOHAMED A. EL GHARBAWI e-mail: elgharma2 @yahoo.com Web Site: WWW.dr-elgharbawi.com. Embryology, Anatomy & Physiology of Thyroid gland Congenital Anomalies of Thyroid Definition & Classification of Goiter Diagnosis of a thyroid swelling

E N D
DISEASES OF THYROID GLAND 1 ByPROFESSOR \ MOHAMED A. EL GHARBAWIe-mail: elgharma2 @yahoo.comWeb Site: WWW.dr-elgharbawi.com
Embryology, Anatomy & Physiology of Thyroid gland Congenital Anomalies of Thyroid Definition & Classification of Goiter Diagnosis of a thyroid swelling Simple Goiter (Types, etiology, clinical picture & management) Nodular goiter( Solitary & Multinodular) ILOS, BY END OF THIS LECTURE YOU WILL KNOW
A downgrowth bud from median ectoderm of 1st & 2ndpharyngeal pouches is called the thyroglossal duct. It migrates to just below the thyroid cartilage. This duct gives isthmus, pyramidal lobe & most of the lateral lobes of the Thyroid. A small part at periphery of each lobe is derived from 4th branchial arch Foramen caecum at base of tongue (ant.2/3 & posterior 1/3) indicates attachment of Thyroglossal duct EMBRYOLOGY OF THYROID
After formation of the thyroid gland, the duct obliterates forming the thyroglossal tract which absorbs Remnants of Thyroglossal duct may persist in adults as Thyroglossal Cyst . Arrest of thyroid tissue in the path of the duct may form ectopic thyroid tissue. EMBRYOLOGY OF THYROID
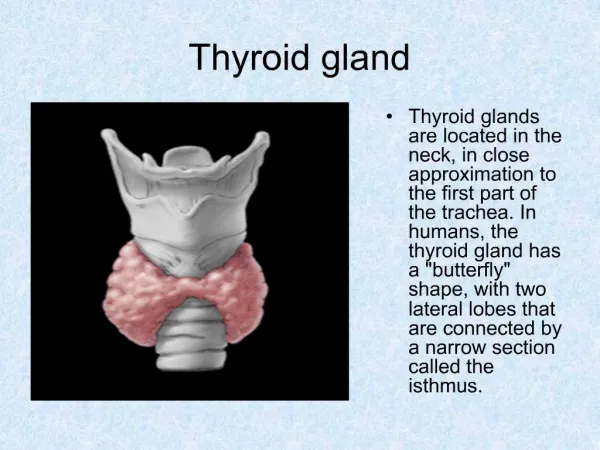
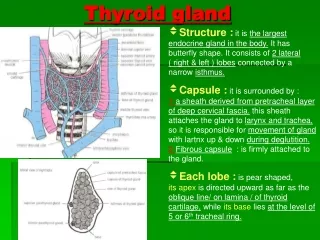
Weight: 15 -25 gms. Butterfly shaped. 2lateral lobes connected by isthmus. Pyramidal lobe is a small angular projection from left upper border of isthmus Upper pole extends from the middle of thyroid cartilage. Lower pole extends to the 5th tracheal ring. ANATOMY OF THYROID GLAND
RELATIONS Posteromedially: related to Larynx, Trachea, Esophagus and Recurrent laryngeal nerve Posterolaterally: Carotid sheath Anteriorly: Skin, SC tissue, Platysma, deep cervical fascia and pre tracheal muscles (Thyrohyoid, sternothyroid & sternohyoid ms. ) Lateral border is overlapped by Sternomastoid ms. ANATOMY OF THYROID GLAND
ATTACHMENTS To trachea by loose areolar tissue Enclosed in the pretracheal fascia (an extension from the deep fascia of the neck), its posteromedial aspect is condensed to form the suspensory ligament of Berry which is attached to trachea & thyroid cartilage This makes the thyroid gland to move up & down with deglutition (movement of the larynx & trachea) ANATOMY OF THYROID GLAND
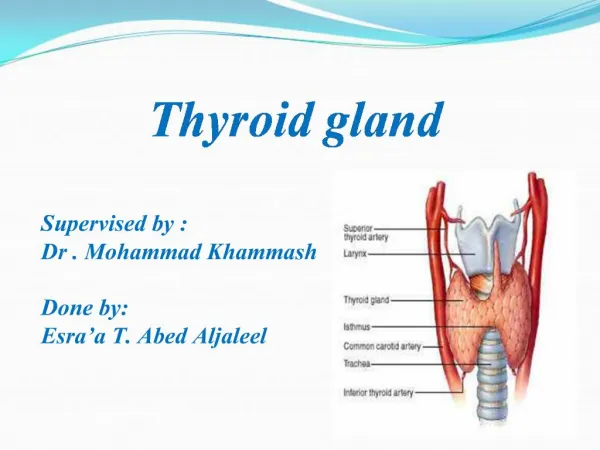
ARTERIAL BLOOD SUPPLY Superior thyroid artery: from external carotid a. Inferior thyroid artery: from the thyrocervical trunk of the subclavian a. (passes behind the carotid sheath infront or behind the recurrentlaryngeal n.) Care during thyroidectomy Thyroidea ima artery: from aortic arch or innominate a. ANATOMY OF THYROID GLAND
VENOUS DRAINAGE Superior& middle thyroid veins: drain internal jugular v. Middle thyroid vein is short and easily rupture during thyroidectomy. It should be ligated early. Inferior thyroid veins run infront of trachea and drain to the innominate vein. ANATOMY OF THYROID GLAND
LYMPH DRAINAGE To the nearby (juxta thyroid) Lymph nodes, then To deep cervical Lymph nodes & Mediastinal Lymph nodes NERVE SUPPLY Sympathetic fibers from the upper 3 cervical ganglia of sympathetic chain pass to the thyroid gland around its arteries. ANATOMY OF THYROID GLAND
THE PARATHROID GLANDS 4 in number. Related to the posteromedial aspect of the thyroid lobes. Usually at points where the superior& inferior thyroid arteries enter the gland. Accidental removal during thyroidectomy leads to postoperative tetany. ANATOMY OF THYROID GLAND
جنيه فضة تذكار كوكب الشرق أم كلثوم 1976
Microscopically, it shows follicles which are normally lined with cubical epithelium. These cells form the colloid to be stored in the lumens of the follicles. Parafollicular C cells are present and secrete Calcitonin. HISTOLOGY OF THE THYROID GLAND
Amino acid Tyrosine attaches to Iodine forming Mono- iodotyrosine. Tyrosine attaches to 2 iodine forming Di- iodotyrosine. 2 di- iodotyrosine combine to form Tetra-iodothyronine (T4) or Thyroxine . Mono-iodotyrosine combines with Di-iodotyrosine to form Tri-iodothyronine (T3) PHYSIOLOGY OF THYROID GLAND
Both T3 &T4 are linked with a specific thyroprotein and stored as intra- acinar colloid. T3 > potent with faster action than T4. T3 & T4 regulate cell metabolism, increase Oxygen consumption & help protein synthesis. Thyrocalcitonin helps in regulation of Calcium metabolism. Its increase leads to hypocalcaemia & vice versa. PHYSIOLOGY OF THYROID GLAND
Thyrotropin Releasing Factor (TRF) from Hypothalamus controls TSH Thyroid Stimulating Hormone (TSH) ; Secreted by the anterior pituitary gland and stimulate the thyroid to form T3& T4 with FEED BACK MECHANISM between both Long Acting Thyroid Stimulator (LATS) is found in 85% of thyrotoxicosis patients. It may be the cause of exophthalmos. Exophthalmos Producing Substance (EPS) is secreted by the anterior pituitary and leads to deposition of retro-orbital fibro-fatty tissue with exophthalmos. PHYSIOLOGY OF THYROID GLAND
ECTOPIC THYROID Ectopic thyroid tissue may be found along course of the thyroglossal tract. Commonly, at base of tongue or foramen caecum. Lingual Thyroid: Presents as a firm nodule at the base of tongue & dating since birth. Big mass may interfere with swallowing, speaking & breathing. Trauma may cause ulceration & bleeding. Congenital Anomalies
ECTOPIC THYROID Investigation : US, Radio-active iodine uptake. Diagnose and localize the ectopic thyroid tissue. Also, get sure that normal thyroid is present. Sometimes, the ectopic thyroid tissue is the only available. To be differentiated from the Lateral aberrent thyroid. Thyroid tissue at the lateral side of neck which is considered now as Secondary in the L N from a small papillary thyroid carcinoma. Treatment: Surgical excision if complications occur. Give replacement thyroxine if it is the only thyroid tissue Congenital Anomalies
CRETENISM It is a congenital thyroid hypofunction. May be associated with aplasia or hypoplasia of the thyroid gland. Also, may be associated with a goitrous gland (Cretinoid Goitre) The child is sluggish and constipated. Looks with puffy face, flat nose, thick lips, protruded tongue, short neck & spade shaped hands (short thick). Congenital Anomalies
CRETINISM Child is quite, rarely cries with delay to learn suckling, walking, speaking & sphincter control In adolescence, the patient is dwarf with supraclavicular pad of fat, skin is dry and wrinkled, mentally retarded, very low BMR and delayed ossification of epiphyses Treatment: Thyroxine (Eltroxine) is a replacement for life Cretinoid goitre : Total thyroidectomy + Thyroxine for life Congenital Anomalies
THYROGLOSSAL CYST This cyst may occur along the course of the thyroglossal tract. A type of tubulodermoids Site: Infrahyoid > suprahyoid Exactly in midline (25% may be little shifted to Lt) Globular, smooth surface, usually firm Not attached to skin (may attach to it if infected) Congenital Anomalies
THYROGLOSSAL CYST Moves up with deglutition and protrusion oftongue (due to the fibrous band extending from the cyst to base of tongue) This fibrous band is related to the middle part of the hyoid bone & may pass through it. Treatment: Dissection & Excision of the cyst and the tract with the middle part of the hyoid bone (Sistrunk’s operation). Congenital Anomalies
THYROGLOSSAL FISTULA Always acquired due infection or incision of a pre-existing thyroglossal cyst Tiny opening in the middle line of the neck, discharge may be serous fluid or mucopurulent The opening moves up with deglutition and protrusion of the tongue. May be inverted due to traction of the fibrous tract on the skin Congenital Anomalies
THYROGLSSAL FISTULA A fibrous band (tract) can be felt extending up from the fistula. It is adherent to the hyoid bone, passing through or behind it. Treatment: Excision of the fistula with whole tract to the base of the tongue & middle part of hyoid bone (Sistrunk’s operation). Otherwise, it will recur. Congenital Anomalies
Definition: Now, it is a enlargement of thyroid gland what ever its cause. Old definition: Non-inflammatory, non-neoplastic enlargement of thyroid gland. Classification: I. Simple goiterII . Toxic goiterIII. Neoplastic goiterIV. Inflammatory goiter GOITRE (GOITER)
DIAGNOSIS OF THYROID SWELLING CLINICAL EXAMINATION: A Mostly butterfly swelling in front of neck at anatomical site of thyroid gland.Moves up & down with deglutition (pretachel fascia), except if it is very huge, retrosternal or fixed to surrounding tissues with advanced malignancy.Doesn’t move with protrusion of the tongue GOITRE (GOITER)
INSPECTION (Butterfly, In front of neck, Suprasternal notch disappear)
Moves with deglutition (Checked by inspection & palpation)