Download
1 / 33
330 likes | 449 Views
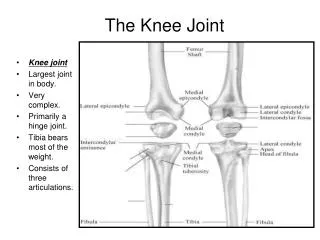
Knee Injury – Distance Running. Dwan Perry, DO Mary L. Ireland, MD. An Equal Opportunity University. History. ID: 37 year-old male Sport: Former collegiate cross country athlete, current recreational runner CC: Right Knee Pain. An Equal Opportunity University. History.

E N D
Knee Injury – Distance Running Dwan Perry, DO Mary L. Ireland, MD An Equal Opportunity University
History • ID: 37 year-old male • Sport: Former collegiate cross country athlete, current recreational runner • CC: Right Knee Pain An Equal Opportunity University
History • HPI: Insidious onset of intermittent, sharp right knee pain over the last month An Equal Opportunity University
History • Competes in several races per year • Reports a recent increase in mileage averaging 12-13 mi/day • Onset of medial sided knee pain with runs and prolonged walking • Has tried cryotherapy and over-the-counter analgesics with mild relief An Equal Opportunity University
History • Denies recent trauma, swelling, or radiating symptoms • No recent changes in shoes, running style or surface An Equal Opportunity University
History • Past Medical History: None • Past Surgical History: None • Social History: Employed full time as a physician, non-smoker, no illicit drug use • Medications: OTC NSAIDs PRN • Allergies: None An Equal Opportunity University
Physical Exam • Athletic white male in no acute distress • Tenderness to palpation over the medial tibial plateau just proximal to the pes anserine tendon insertion • No joint line tenderness or palpable effusion • Full ROM at the knee An Equal Opportunity University
Physical Exam • No significant pain with resisted knee flexion or extension • Neurovasularly intact distally • Negative Lachman’s, McMurray’s, anterior and posterior drawer testing, Stable to varus and valgus stress (0°/30°) • Otherwise, normal exam of the BLE An Equal Opportunity University
Imaging • Radiographs of the Bilateral Knee: 1. No evidence of fracture or loose bodies. • MRI of the Right Knee without Contrast: 1. Reactive bone marrow edema in the medial tibial plateau without overlying meniscal tear or significant cartilage loss. 2. Irregular edema within the fibular head indicative of early arthrosis affecting the proximal tibiofibular articulation An Equal Opportunity University
T2 Axial A1#19, 20, 21, 22 An Equal Opportunity University
T2 Coronal A2#13, 14, 15, 16 An Equal Opportunity University
T2 Sagittal A4#14, 15 16, 17 An Equal Opportunity University
Discussion An Equal Opportunity University
Differential Diagnosis 1. Medial Meniscus Injury 2. Tibial Stress Fracture 3. Articular Cartilage Defect of the Medial or Patellofemoral Compartment 4. Pes Anserine Bursitis An Equal Opportunity University
Final Diagnosis Anteromedial Proximal Tibial Plateau Stress Fracture An Equal Opportunity University
Treatment and Outcomes • Cessation of the painful activities • Gradual return to running once asymptomatic • Upon return to running, pain returned • Another period of relative rest An Equal Opportunity University
Treatment and Outcomes • After resolution of pain, the patient was able to return to running with no recurrence of pain at one year after initial presentation. An Equal Opportunity University
Discussion An Equal Opportunity University
Stress Fractures • Repetitive and excess stress • Acceleration of normal bone remodeling • Microfractures Stress Reaction Stress Fractures • Imbalance of bone repair • Caused by intrinsic and extrinsic factors An Equal Opportunity University
Risk Factors • Intrinsic Factors • Metabolic state (Vit D, EA, etc) • Menstrual patterns • Fitness level • Anatomic alignment • Microscopic bone structure • Bone vascularity An Equal Opportunity University
Risk Factors • Extrinsic factors • Training regimen • Dietary habits • Equipment An Equal Opportunity University
Location • Tibia (23.6%) • Tarsal Navicular (17.6%) • Metatarsal (16.2%) • Fibula (15.5%) • Femur (6.6%) • Pelvis (1.6%) • Spine (0.6%) An Equal Opportunity University
Who does this effect • Repetitive, HIT (athletes, military recruits) • Recreational Runners (25 mi/week) • W >M • Low Bone Mineral Density • Smokers • Greater than 10 EtOH drinks per week An Equal Opportunity University
History • Insidious onset of pain • Recent change in training habits or equipment • Dietary hx (Ca, Vit D, Prot, ETOH, caffeine) • PMH of endocrinopathies, autoimmune d/o, eating d/o, depression, GERD An Equal Opportunity University
Physical Exam • Tenderness over the affected bone • Hop Test (Tibia) • Fulcrum Test (Femur) • Spinal Extension Test (Pars) • Bradycardia, orthostatic hypotension, and stigmata of eating disorders An Equal Opportunity University
Differential Dx • Vary based on location • Tendinopathy • Compartment Syndrome • MTSS • Malignancy An Equal Opportunity University
Imaging • Plain XRs • Acuity of injury • Cortical bone involvement • Early: subtle radiolucency or poor cortex definition • Late (weeks to months): Sclerosis of endosteum and periosteal elevation • Cancellous bone involvement • Band of sclerosis perpendicular to trabeculae An Equal Opportunity University
Imaging • Plain XRs • Findings lag by weeks • May repeat in 2 wks to see fracture An Equal Opportunity University
Imaging • MRI • Fluid sensitive sequences helpful • Show endosteal marrow and periosteal edema • Bone Scan • Increased uptake within days to weeks An Equal Opportunity University
Imaging • US • Good for relatively superficial bones • Step-off • Hypoechoic band • Periosteal reaction • Hyperechoic callus formation • Hypervascularity with PDI An Equal Opportunity University
Lab Workup • CBC/CMP • Vit D • TSH/PTH • ESR • UPT, Prolactin, Estradiol, FSH, LH • If suspect Female Athlete Triad An Equal Opportunity University
Treatment • Nonsurgical • Rest and immobilization • Vit D/Ca supplement if necessary • Biphosphonates controversial • Surgical • For high risk Fx (Fem neck, Ant Tib, Navicular, Talus, Prox 2nd MT, Pars) An Equal Opportunity University
Thank You An Equal Opportunity University