Download

1 / 25
260 likes | 286 Views
Explore the physiology of erection, mechanisms, and treatment options for male sexual dysfunction in relation to diabetes. Learn about the epidemiology and impact on both genders.

E N D
Sexual dysfunction &Diabetes S. Vahidi M.D.
Male sexual dysfunction • Inability to achieve a satisfactory sexual relationship • Inadequacy of erection • Problem with emission, ejaculation or orgasm
Physiology of Erection Innervation of the penis • Autonomic T12- l2 (sympathetic ) & S2 S4(parasympathetic) Inferior hypogastric & pelvic plexus Pelvic organ: Cavernous nerve • Somatic Sensory: pain- temperature- touch- vibratory Thalamus Motor: S2-S4+ pudendal nerve Bulbo cavernous M. Ischiocavernous M. • Supraspinal Forebrain Brain stem Hypaothalamus Midbrain The brain has a modulatory effect on the spinal pathway of erection.
Erection types • Genital stimulated (contact or reflexogenic) • Central-stimulated (non contact or psychogenic) • Central originated (nocturnal) (in REM period)
Physiology of erection Hemodynamic • Artery: internal pudendal • Bulbo urethral • Dorsal a. • Covernous a. (deep a.) • Vein: • Deep dorsal vein (glans- corporacovernosa) • Circumflex- urethral- bulbar vein (corpus spongiosum) • Cavernous- crural vein- deep dorsal vein (corpora cavernousa)
Phases of erection process • Flaccid Ph. • Latent (filling) Ph. • Tumescent Ph. • Full erection Ph. • Rigid erection Ph. • Detumescent Ph.
Hormons and sexual function • Androgens are essential for male sexual maturity • Androgens enhances but are not essential for erection
Neuro transmitters and erection • Adrenergic flaccid • Cholinergic (No) erection • Non adrenergic non cholinergic (No) erection • Prostaglandins- endothelins and angiotensin
Male sexual dysfunction • Inability to achieve a satisfactory sexual relationship • Inadequacy of erection • Problem with emission, ejaculation or orgasm
Epidemiology of E.D. • 52% of male between 40 and 70 years have E.D. • 17% mild E.D. • 25% moderate E.D. • 10% complete E.D. • The major predictor of E.D • Diabetes mellitus • Heart disease • Hypertension • ↓HDL
Diabetes mellitus, although the most common endocrinologic disorder cause E.D. through its vascular, neurologic, endothelial and psychogic complications rather than hormon deficiency per se. Failure to initiate = neurogenic Failure to file= arterial Failure to store= venous Classification of E.D.
Diabetes & E.D. • About 50% of men with chronic D.M. have E.D. • E.D has been estimated to occur in 35% to 75% of men with D.M. • Deterioration of sexual function was the first symptom in 12% of D.M. • The prevalence of E.D is three times higher in diabetic men (28% versus 9.6%) • E.Doccurs at an earlier age and increases with disease duration in D.M. • The incidence of E.D in D.M. is age dependent • 15% at age 30 • 55% at age 34-60
Diabetes & E.D. • Diabetes may cause E.D. through its effect on CNS peripheral nerve function, androgen production, psychological factors vascular integrity, and endothelial and smooth muscle function. • There is no correlation between insulin dosage, duration of disease, the effectives of disease control and E.D.
Identify the cause of E.D • Intra cavernosal inj • Duplex scanning • Cavernosometry and cavernosography • Arteriography • NPT • Rigiscan
Treatment of E.D • Lifestyle changes • Changing medications • Psychosexual therapy • Hormonal therapy • Phosphodiesterase inhibitors (sildenafil) • Yohimbin – trazodone- apomorphine • Trans urethral therapy • Intra cavernous injection Papaverin- phentolamin- prostaglandin E1 • Vacuum device • Vascular surgery • Penile prosthesis
Disorders affecting emission, ejaculation & orgasm • Premature ejaculation • Retrograde ejaculation • Dry ejaculation
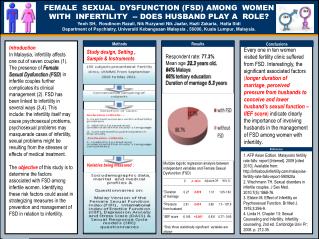
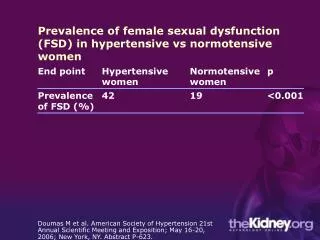
Female sexual dysfunction & diabetes • Diabetes metabolic problem loss of desire • Diabetes psychologic problem loss of desire • Strong correlation between depression & F.S.D. in diabetic with neuropathy. • F.S.D. in diabetic: orgasm- arousal- painful orgasm- desire- lubricant problem