Download
1 / 33
330 likes | 1.33k Views
Embryogenesis of the Kidneys and Ureters. Normal Development. Three excretory organs (pronephroi, mesonephroi, and metanephroi) develop from the intermediate mesoderm

E N D
Normal Development • Three excretory organs (pronephroi, mesonephroi, and metanephroi) develop from the intermediate mesoderm • However, since pronephroi are never functional in human embryos and degenerate on days 24 or 25, we will present only the concepts of mesonephroi and metanephroi
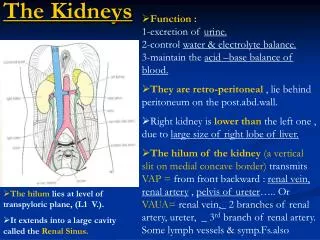
A. A pair of cervical nephrotomes forms in each of five to seven cervical segments, but these quickly degenerate during the 4th week. B The mesonephric ducts first appear on day 24 C. Mesonephric nephrotomes and tubules form in craniocaudal sequence throughout the thoracic and lumbar regions. D. The mesonephroi contain functional nephric units consisting of glomeruli, Bowman's capsules, mesonephric tubules, and mesonephric ducts.
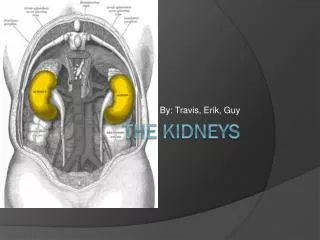
Ventral views of the abdominopelvic region of embryos and fetuses (sixth to ninth weeks), showing medial rotation and 'ascent' of the kidneys from the pelvis to the abdomen.
Congenital Anomalies A. Unilateral renal agenesis. B. Right side, pelvic kidney; left side, divided kidney with a bifid ureter
The left kidney crossed to the right side and fused with the right kidney C. Right side, malrotation of the kidney; left side, bifid ureter and double kidney. D. Crossed renal ectopia.
E. 'Pancake' or discoid kidney resulting from fusion of the kidneys while they were in the pelvis. F. Supernumerary left kidney resulting from the development of two ureteric buds.
Common congenital anomalies of the kidney • Agenesis of the kidney • Hypoplasia & dysplasia • Supernumerary kidney • Horse – shoe kidney • Cystic disorders • Medullary sponge kidney
Horseshoe Kidney Diagnosed by IVU • Horseshoe kidney is the most common type of fusion, occurring in 1 in 400, with 90% fused at the lower poles. • Associated with urogenital anomalies and an increased incidence of renal pelvic tumors. • One third of patients remain asymptomatic, whereas others may present with symptoms of hydronephrosis [ureteropelvic junction (UPJ) obstruction], infection, or stones
Renal Hypoplasia • Hypoplasia refers to reduced renal mass (i.e., fewer than normal cells or nephrons) without histologic evidence of dysplasia
Renal Dysplasia • Dysplasia is a form of abnormal renal morphogenesis characterized histologically by primitive ducts and cartilage. • Most hypodysplastic kidneys have ectopic ureteral orifices. • The more ectopic the orifice, the greater the degree of dysplasia
Cystic disorders of the kidney • Quite common • Polycystic kidney disease: bilateral condition • Medullary sponge kidney • Solitary renal cyst
Polycystic kidney disease • Cystic genetic disorder of the kidney • Associated with cysts in the liver, pancreas, brain & heart • Types: • Autosomal dominant • Autosomal recessive
Autosomal dominant polycystic kidney disease • Late onset • Due to mutations in either the PKD-1 or PKD-2 gene.
Autosomal recessive polycystic kidney disease • Early onset • Less common than ADPKD
Clinical features • Abdominal lump • Pain • Haematuria • Hypertension • Infection • Uraemia
Investigations • USG • Excretory urograms
Complications • Pyelonephritis • Infection of cysts • Renal failure
Treatment • Conservative: low protein diet, increased intake of fluid • Surgery: • Rovsing’s operation
Congenital Multicystic Kidney Disease • Congenital multicystic kidney disease is a common benign dysplastic malformation of the fetal kidney secondary to obstruction from ureteropelvic occlusion, ureteral atresia, or agenesis • Elective surgical excision is indicated if the mass interferes with respiration or alimentation
Medullary Sponge Kidney • Medullary sponge kidney is a congenital deformity of the renal medulla consisting of multiple, puddle-like dilatations of the collecting ducts in the papillae on IVU(fan-shaped pyramidal blush ) • The disease is bilateral in 75% of patients. • Predisposition to calcium phosphate nephrolithiasis in the adult, presenting with renal colic and hematuria secondary to stone passage. • Treatment consists of preventing infection and stone formation.
Congenital anomalies of the ureter • Absence of one ureter • Duplication of ureter • Ureterocele
Ectopic Ureter • An ectopic ureter is one that opens in some location other than the bladder. • Most common sites for insertion of the ectopic orifice in female patients are the urethra, vestibule, and vagina, and present as urinary incontinence. • Most common sites for insertion of the ectopic orifice in male patients are the posterior urethra and seminal vesicles, often remaining unrecognized until late in life. • partial nephroureterectomy of the nonfunctioning upper-pole component or pyelopyelostomy with only a distal ureterectomy if the upper pole functions.
Ureterocele • A ureterocele is a congenital cystic ballooning of the terminal submucosal ureter. • It is classified as or • Simple----represents about 30% of all ureteroceles and occurs primarily in adult , present with infection • Ectopic--- 70% of all ureteroceles,in female, with a left predominance; 10% are bilateral • Prenatal ultrasound ,IVU • Excision and reimplantation of the distal ureter, • A complete nephroureterectomy may be necessary if the entire kidney is nonfunctional
Megaureter • Megaureter is a term that most urologists use to refer to primary ureteral dilatation in the absence of extraureteral disease • Most children with megaureter will present with urinary tract infection, hematuria, or a flank mass; 25% of cases are bilateral. • USG, IVU
Classification • Obstructed megaureter --secondary to urethral obstruction as with valves, prolapsing ureterocele, calculi, granulomatous disease, or other extrinsic causes; • Refluxing megaureter is from either primary intrinsic ureteral reflux or reflux secondary to bladder-outlet obstruction or neurogenic bladder; • Nonrefluxing, nonobstructed megaureter is a congenital idiopathic ureteral dilatation often associated with megacalycosis
Treatment • Most patients with primary megaureter have the nonrefluxing, nonobstructing type that needs no surgical intervention • Primary obstructive megaureter requires surgical correction, commonly by tapering the lowermost 5 cm of ureter with reimplantation