Download
1 / 48
490 likes | 658 Views
The Health Policy Process. Andy Bindman, MD Professor Medicine, Health Policy, Epidemiology & Biostatistics UCSF. Format of Class. Primarily lectures with some discussion and in class exercises Great guest speakers Karin Rush-Munroe Rebecca Smith-Bindman Cathy Hoffman Andy Schneider

E N D
The Health Policy Process Andy Bindman, MD Professor Medicine, Health Policy, Epidemiology & Biostatistics UCSF
Format of Class Primarily lectures with some discussion and in class exercises Great guest speakers Karin Rush-Munroe Rebecca Smith-Bindman Cathy Hoffman Andy Schneider Drew Altman
Grading Policy Based on homework assignments and class participation No final exam Homework due via email to Khoa Nguyen the Monday evening (6 PM) following each class Homework intended to extend from your own area of research
Policy Experience How many have lived in DC?
Policy Experience How many have lived in DC? How many have participated in a political campaign?
Policy Experience How many have lived in DC? How many have participated in a political campaign? How many have worked for an elected official?
Policy Experience How many have lived in DC? How many have participated in a political campaign? How many have worked for an elected official? How many have received a political appointment?
Policy Experience How many have lived in DC? How many have participated in a political campaign? How many have worked for an elected official? How many have received a political appointment? How many have held elective office?
Policy Experience How many have lived in DC? How many have participated in a political campaign? How many have worked for an elected official? How many have received a political appointment? How many have held elective office? How many want to run for elective office?
Policy What government does Making decisions, discretion, unstructured, consequential What government chooses to do and what not to do
Major Health Policy Domains Public health Research Workforce Financing health care
Federal Health Policy Agencies Public health CDC, FDA Research NIH, AHRQ Workforce HRSA Financing health care CMS
Health Policy Extends Beyond Federal Level Federal Medicare, VA, Tricare State Medicaid, CHIP Insurance Exchange Local Indigent care including immigrants
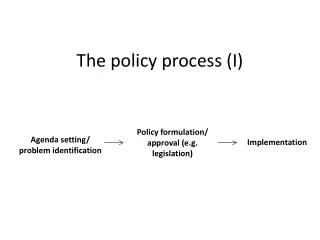
Policy Process Problem recognized Policy developed to deal with problem Law created Law implemented
Role of Research in Policy Process Problem identified with help of research Decision making about actions supported by research on options Policy implemented Monitoring and evaluation through research Research at the core of rational decision making based on consideration of all the options
Policy Process Not Quite So Evidence Based Real life decision making not linear More iterative process Too complex to consider all the options and insufficient data to do so Rather than finding ideal solution policymakers looking for a “good enough” one
Incremental Policy “Good enough solutions” lead to small scale changes Research not at the heart of assessing all the options but used in selective ways by competing groups that move in a diffuse way toward consensus
Who Brings Problems to Policymakers’ Attention? Constituents Researchers Journalists Special interest groups
How Do Policymakers Arrive at Their Beliefs Respectful of scientists and health professionals but not reliant on evidence-based research Politicians talk to a range of stakeholders to form their sense of the truth More similar to journalism than science
Why Isn’t Research More Convincing to Policymakers? Research often more narrowly defined than range of policy options Rarely available in a way that is both generalizable to the nation and specific to an area Data are often old by the time they are available Lots of competing data and policymakers don’t have much ability to distinguish among them
Prerequisites for Government Action Identification of a social problem Must be persuaded that problem requires government intervention Must have a method for how the government can respond to bring about desired change
Is It a Public Problem Is the problem better solved through policy or can it be resolved through the profession? Or the marketplace? Ideological debate about role of government Profession given a significant amount of autonomy for policing its members
25% of Implanted Defibrillators are Unnecessary - JAMA Should this be corrected by The profession through education? The marketplace by educating consumers about cardiologists’ performance? Medicare not paying for inappropriate defibrillators? Government suing manufacturers who promote “off label” use of defibrillators and providers who repeatedly insert them in patients without clear indication
Political Context Punctuated equilibrium - long periods of stability punctuated by occasional major change Coupling of a policy window of opportunity with a solution
Who Makes Federal Health Policy? Iron Triangle Administration Senate House of Representatives
The Administration Executive Office of the President Office of Domestic Policy Office of Management and Budget Health and Human Services
The Congress Agenda setting in each chamber Senate Majority Leader Speaker of the House Committees Senate Finance and HELP Committees House Energy and Commerce, Ways and Means, Education and Labor
Who Develops the Policy? Staff working on behalf of elected members of Congress Interplay between Congressional staff in Senate and House with guidance from White House staff
Policy Lifecycle Identified problem Broad demand for action Realization of costs Difficulties and opposition
Who Figures Out the Cost Congressional Budget Office (CBO) Non partisan Congressional think tank Highly skilled economists Federal costs Not cost effectiveness Model not subject to peer review Disseminates results on website www.cbo.gov
Impediments to Change Interest groups support the policy legacy - often maintaining a status quo they would not have chosen in first place
Dance of Legislation Typically legislation evolves through subcommittees, and full committees of jurisdiction before full chamber level votes “Hearings” and “Mark-ups” If multiple committees of jurisdiction then bills must be merged before chamber votes House and Senate must pass the same version of bill and President must sign to become law
Congress’s Decision-Making Process Much more tortured and drawn out than clinical decisions Visited and revisited with each member Requires lots of face time Voting influenced by how member perceives re-election, power relationships in chamber, and quality of the policy
Intended and Unintended Consequences of Policies Law often purposely ambiguous Laws create winners and losers Start and end dates can create policy “cliffs”
Implementation Executive branch interprets law and writes regulations; interpretations can vary Opponents can challenge parts or all of a law in court as unconstitutional Congress can influence by providing or withholding funds to implement If requires state or local government cooperation they can introduce variation in implementation
Role of Research in Health Policy Identify problems in need of solution To provide evidence regarding policy options To monitor/evaluate whether policy is achieving goals
My Research and Its Connection with Policy Long standing interest in access to care for low income populations Focus on the effectiveness of Medicaid. the largest public health insurance program for the poor Does Medicaid coverage provide adequate access to care?
Some of My Research Findings For the general population, many California counties have a shortage of primary care physicians These shortages are greater for Medicaid beneficiaries than the privately insured In repeated studies over 15 years only half of primary care physicians in California accept Medicaid patients in their practice Main reason cited by physicians for not participating in Medicaid is poor reimbursement
Related Research of Others Nationally about 60% of primary care physicians accept new Medicaid patients Primary care payment rates across states average about 60% of Medicare States that have significantly improved their primary care payment rates have seen an increase in participation
Why Is This A Problem in Need of a Federal Policy Fix Physician participation in Medicaid is optional Problem has been persistent and not corrected by market forces Profession does not advocate for physician participation in Medicaid States determine provider payment rates and in a context in which they are not held accountable for access they have a financial interest in paying low rates
Window of Opportunity Health reform increasing population in Medicaid by 16 million Reports from Massachusetts that insurance expansion worsened rather than improved ED overcrowding because of inadequate access to primary care Large Democratic states have some of the lowest Medicaid physician participation and payment rates
Proposed Policy Solution Require states to reimburse Medicaid primary care visits at Medicare rates Federal government to provide funds for difference between a state’s current rate and the Medicare rate CBO estimated it would cost $57 billion to bring Medicaid provider payments to Medicare rates over next 10 years
Opposition Too costly Not all convinced that Medicaid beneficiaries have an access barrier or that paying physicians more will solve Payment and participation in Medicaid tends to be less of a problem in rural states House approved $57 billion; Senate $0
Compromise:Winners, Losers and Cliffs Cost reduced to $10 billion Provision narrowed to cover only primary care (GIM, Peds and FM) Federal funding guaranteed for only 2013-2014 then a cliff
Evaluating Whether Policy is Achieving Goal State survey over time to monitor whether primary care physician participation in Medicaid changes in association with increased payment Using specialist participation in Medi-Cal over time as a comparison group
Homework Assignment Describe your research Develop an argument for why your research supports a change in policy - government action Extra credit for saying level of government and entity of government who could lead the change and why