Download
1 / 1
10 likes | 153 Views
Table 2. Timing of ADP receptor inhibitor switch. Unplanned 30-Day Readmission Risk Among Patients with Acute Myocardial Infarction: a Report from TRANSLATE-ACS Connie N. Hess, MD 1 ; Tracy Y. Wang, MD, MHS 1 ; Lisa McCoy 1 ; Emily Honeycutt 1 ;

E N D
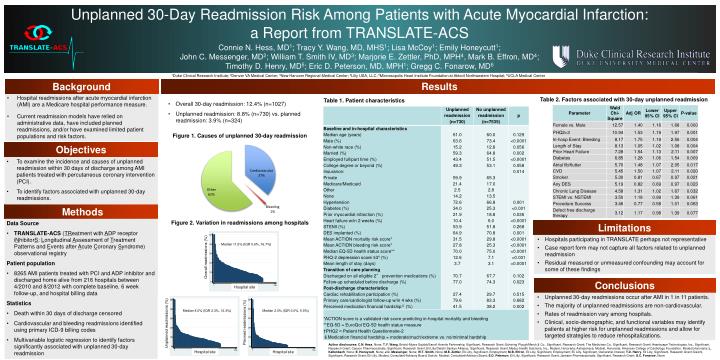
Table 2. Timing of ADP receptor inhibitor switch Unplanned 30-Day Readmission Risk Among Patients with Acute Myocardial Infarction: a Report from TRANSLATE-ACS Connie N. Hess, MD1; Tracy Y. Wang, MD, MHS1; Lisa McCoy1; Emily Honeycutt1; John C. Messenger, MD2; William T. Smith IV, MD3; Marjorie E. Zettler, PhD, MPH4, Mark B. Effron, MD4; Timothy D. Henry, MD5; Eric D. Peterson, MD, MPH1; Gregg C. Fonarow, MD6 1Duke Clinical Research Institute; 2Denver VA Medical Center; 3New Hanover Regional Medical Center; 4Lilly USA, LLC; 5Minneaopolis Heart Institute Foundation at Abbott Northwestern Hospital; 6UCLA Medical Center Results Background • Hospital readmissions after acute myocardial infarction (AMI) are a Medicare hospital performance measure. • Current readmission models have relied on administrative data, have included planned readmissions, and/or have examined limited patient populations and risk factors. Table 2. Factors associated with 30-day unplanned readmission Table 1. Patient characteristics • Overall 30-day readmission: 12.4% (n=1027) • Unplanned readmission: 8.8% (n=730) vs. planned readmission: 3.9% (n=324) Figure 1. Causes of unplanned 30-day readmission Objectives • To examine the incidence and causes of unplanned readmission within 30 days of discharge among AMI patients treated with percutaneous coronary intervention (PCI). • To identify factors associated with unplanned 30-day readmissions. Methods Figure 2. Variation in readmissions among hospitals • Data Source • TRANSLATE-ACS (TReatment with ADP receptor iNhibitorS: Longitudinal Assessment of Treatment Patterns and Events after Acute Coronary Syndrome) observational registry • Patient population • 8265 AMI patients treated with PCI and ADP inhibitor and discharged home alive from 216 hospitals between 4/2010 and 8/2012 with complete baseline, 6 week follow-up, and hospital billing data • Statistics • Death within 30 days of discharge censored • Cardiovascular and bleeding readmissions identified using primary ICD-9 billing codes • Multivariable logistic regression to identify factors significantly associated with unplanned 30-day readmission Limitations • Hospitals participating in TRANSLATE perhaps not representative • Case report form may not capture all factors related to unplanned readmission • Residual measured or unmeasured confounding may account for some of these findings Median 11.5% (IQR 5.6%, 16.7%) Overall readmissions (%) Unplanned readmissions (%) Conclusions Hospital site • Unplanned 30-day readmissions occur after AMI in 1 in 11 patients. • The majority of unplanned readmissions are non-cardiovascular. • Rates of readmission vary among hospitals. • Clinical, socio-demographic, and functional variables may identify patients at higher risk for unplanned readmissions and allow for targeted strategies to reduce rehospitalizations. Hospital site Median 2.0% (IQR 0.0%, 5.9%) Median 8.0% (IQR 2.3%, 12.3%) Planned readmissions (%) Author disclosures: C.N. Hess, None; T.Y. Wang, Bristol-Myers Squibb/Sanofi Aventis Partnership, Significant, Research Grant; Schering Plough/Merck & Co., Significant, Research Grant; The Medicines Co., Significant, Research Grant; Heartscape Technologies, Inc., Significant, Research Grant; Canyon Pharmaceuticals, Significant, Research Grant; Eli Lilly/Daiichi Sankyo Alliance, Significant, Research Grant; Medco Health Solutions, Inc., Modest, Honoraria; Astrazeneca, Modest, Honoraria; American College of Cardiology Foundation, Modest,Honoraria; L. Kaltenbach, None; E. Honeycutt, None; J.C. Messenger, None; W.T. Smith, None; M.E. Zettler, Eli Lilly, Significant, Employment; M.B. Effron, Eli Lilly, Significant, Employment; Eli Lilly, Significant, Ownership Interest; T.D. Henry, Eli Lilly, Significant, Research Grant; Daiichi, Significant, Research Grant; Eli Lilly, Modest, Consultant/Advisory Board; Daiichi, Modest, Consultant/Advisory Board; E.D. Peterson, Eli Lilly, Significant, Research Grant; Janssen Pharmaceuticals, Significant, Research Grant; G.C. Fonarow, None. Hospital site