Download
1 / 38
560 likes | 2.4k Views
Acute Respiratory Distress Syndrome. Alice Gray, MD Duke University Medical Center March 21, 2007. Objectives. Define ARDS and describe the pathological process Know causes of ARDS, and differential diagnosis Understand specific challenges in mechanical ventilation of patients with ARDS

E N D
Acute Respiratory Distress Syndrome Alice Gray, MD Duke University Medical Center March 21, 2007
Objectives • Define ARDS and describe the pathological process • Know causes of ARDS, and differential diagnosis • Understand specific challenges in mechanical ventilation of patients with ARDS • Understand treatment strategies and evidence behind them
ARDS • First described 1967 by Ashbaugh and colleagues • Severe lung injury characterized by non-cardiogenic pulmonary edema, decreased lung compliance, refractory hypoxemia • 1994 Consensus Definition • Acute onset (<2 weeks) • Bilateral infiltrates on chest xray • PCWP ≤18mmHg or lack of evidence of left atrial hypertension • Acute lung injury if PaO2/FiO2 ≤300 • ARDS if PaO2/FiO2 ≤200
Epidemiology • Incidence of acute lung injury (ALI): 17.9-78.9 cases per 100,000 person-years • Incidence of acute respiratory distress syndrome (ARDS): 13.5-58.7 cases per 100,000 person-years • Approx 9% of ICU beds in US N Engl J Med. 2005;353:1685-93. Am J Respir Crit Care Med. 1999;159:1849-61.
Most common causes ARDS • Pneumonia (34%) • Sepsis (27%) • Aspiration (15%) • Trauma (11%) • Pulmonary contusion • Multiple fractures ARDSnet NEJM 2000:342:1301-8.
Causes of ARDS NEJM 2000;342,18:1334-1349
Risk factors for ARDS • Preexisting lung disease • Chronic alcohol use • Low serum pH • Sepsis • 40% of patients with sepsis develop ARDS
Pulmonary edema from left heart failure Diffuse alveolar hemorrhage Acute eosinophilic pneumonia Lupus pneumonitis Acute interstitial pneumonia Pulmonary alveolar proteinosis BOOP or COP Hypersensitivity pneumonitis Leukemic infiltrate Drug-induced pulmonary edema and pneumonitis Acute major pulmonary embolus Sarcoidosis Interstitial pulmonary fibrosis Differential diagnosis
Excluding other diagnoses • Echo • Central venous catheter • Bronchoscopy with bronchoalveolar lavage (to eval for hemorrhage, AEP, etc) • Chest CT
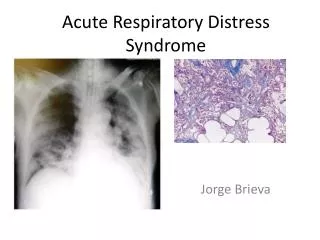
Acute (Exudative) Phase • Rapid onset respiratory failure in patient at risk for ARDS • Hypoxemia refractory to oxygen • Chest xray resembles cardiogenic pulmonary edema • Bilateral infiltrates worse in dependent lung zones, effusions • Infiltrates may be asymmetric
Acute Phase - Radiographs NEJM 2000;342,18:1334-1349
Pathological findings • Diffuse alveolar damage • Neutrophils, macrophages, erythrocytes • Hyaline membranes • Protein-rich edema in alveolar spaces
Acute (Exudative) Phase Alveolar Filling Expansion of interstitium with macrophages and inflammation Hyaline Membranes
Fibroproliferative Phase • Persistent hypoxemia • Fibrosing alveolitis • Increased alveolar dead space • Decreased pulmonary compliance • Pulmonary hypertension • From obliteration of capillary bed • May cause right heart failure
Fibroproliferative phase • Chest xray shows linear opacities consistent with evolving fibrosis • Pneumothorax in 10-13% of patients • CT: diffuse interstitial opacities and bullae • Histologically, fibrosis, mesenchymal cells, vascular proliferation, collagen and fibronectin accumulation • Can start 5-7 days after symptom onset • Not present in every patient with ARDS, but does portend poorer prognosis
Fibroproliferative phase NEJM 2000;342,18:1334-1349
Fibrosing alveolitis NEJM 2000;342,18:1334-1349.
Recovery phase • Gradual resolution of hypoxemia • Hypoxemia improves as edema resolves via active transport Na/Cl, aquaporins • Protein removal via endocytosis • Re-epithelialization of denuded alveolar space with type II pneumocytes that differentiate into type I cells • Improved lung compliance • Chest xray and CT findings resolve • PFTs improve, often normalize
Management of ARDS • Treat underlying illness • Sepsis, etc • Nutrition • Supportive care • DVT prophylaxis • GI prophylaxis • Medications
Complications in Managing ARDS patients • Mechanical ventilation causes: • Overdistention of lungs (volutrauma) • Further damaging epithelium • Increased fluid leak, indistinguishable from ARDS damage • Barotrauma • Rupture alveolar membranes • Pneuomothorax, pneumomediastinum • Sheer stress • Opening/closing alveoli • Inflammatory reaction, cytokine release • Oxygen toxicity • Free radical formation
ARDS Network • NIH-funded consortium of 10 centers, 24 hospitals, 75 intensive care units • Goal to design large RCTs to determine effective treatments • Key ARDSnet studies: • Ventilator volumes • Steroids • PEEP • Volume management/PA catheter
Pulmonary artery catheters • Often used to help evaluate for cardiogenic pulmonary edema • SUPPORT trial (retrospective study) first raised doubts about utility • Two multicenter RCTs confirmed lack of mortality benefit of PA catheters in ARDS (ARDSnet FACTT) • Monitoring CVP equally effective, so PAC not recommended in routine management JAMA. 1996;276:889-97. N Engl J Med. 2006:354:2213-24
Ventilator management – ARDSnet protocol • 861 patients randomized to Vt 10-12 mg/kg ideal body weight and plateau pressure ≤50cmH2O vs Vt 6-8 mg/kg IBW and plateau pressure ≤30cm H2O • KEYS • Low tidal volumes – 6-8mL/kg ideal body weight • Maintain plateau (end-inspiratory) pressures <30cm H20 • Permissive hypercapnia and acidosis • Decreased mortality by 22% NEJM 2000;342:1301-8.
ARDSnet Tidal Volume Study NEJM 2000;342:1301-8.
Positive End-Expiratory Pressure (PEEP) • Titrate PEEP to decrease FiO2 • Goal sat 88% with FiO2 <60% • Minimize oxygen toxicity • PEEP can improve lung recruitment and decrease end-expiratory alveolar collapse (and therefore right-to-left shunt) • Can also decrease venous return, cause hemodynamic compromise, worsen pulmonary edema • ARDSnet PEEP trial of 549 patients show no difference in mortality or days on ventilator with high vs low PEEP NEJM 2004:351(4):327-336
Other Ideas in Ventilator Management • Prone positioning • May be beneficial in certain subgroup, but complications including pressure sores • RCT of 304 patients showed no mortality benefit • High-frequency oscillatory ventilation • In RCT, improved oxygenation initially, but results not sustained after 24 hours, no mortality benefit • ECMO • RCT of 40 adults showed no benefit JAMA 1979;242:2193-6. Am J Respir Crit Care Med. 2002;166:801-8
Drug therapy • Agents studied: • Corticosteroids • Ketoconazole • Inhaled nitric oxide • Surfactant • No benefit demonstrated
Steroids in ARDS • Earlier studies showed no benefit to early use steroids, but small study in 1990s showed improved oxygenation and possible mortality benefit in late stage • ARDSnet trial (Late Steroid Rescue Study “LaSRS” – “lazarus”) of steroids 7+ days out from onset of ARDS • 180 patients enrolled, RCT methylprednisolone vs placebo • Overall, no mortality benefit • Steroids increased mortality in those with sx >14 days JAMA 1998;280:159-65, N Engl J Med 2006;354:1671-84
Steroids in ARDS N Engl J Med 2006;354:1671-84
Other drugs in ARDS • Ketoconazole • ARDSnet study of 234 patients, ketoconazole did NOT decrease mortality, duration of mechanical ventilation or improve lung function • Surfactant • Multicenter trial, 725 patients with sepsis-induced ARDS, surfactant had no effect on 30-day survival, ICU LOS, duration of mechanical ventilation or physiologic function • Inhaled Nitric oxide • 177 patients RCT, improved oxygenation, but no effect on mortality of duration of mechanical ventilation N Engl J Med. 1996;334:1417-21. Crit Care Med. 1998;26:15-23.
Fluid management • “Dry lungs are happy lungs” • ARDSnet RCT of 1000 patients (FACTT), Conservative vs liberal fluid strategy using CVP or PAOP monitoring to guide, primary outcome: death. Conservative fluids • Improved oxygenation • More ventilator-free days • More days outside ICU • No increase in shock or dialysis • No mortality effects
ARDSnet Fluid Management NEJM 2006;354:2564-75.
Keys to management • Treat underlying illness • Supportive care • Low tidal volume ventilation • Nutrition • Prevent ICU complications • Stress ulcers • DVT • Nosocomial infections • Pneumothorax • No routine use of PA catheter • Diuresis/avoidance of volume overload • Give lungs time to recover
Survival and Long Term Sequelae • Traditionally mortality 40-60% • May be improving, as mortality in more recent studies in range 30-40% • Nonetheless survivors report decreased functional status and perceived health • 79% of patients remember adverse events in ICU • 29.5% with evidence of PTSD
1 year after ARDS survival • Lung Function: • FEV1 and FVC were normal; DLCO minimally reduced • Only 20% had mild abnormalities on CXR • Functionally: • Survivors’ perception of health was <70% of normals in: • Physical Role: Extent to which health limits physical activity • Physical Functioning: Extent to which health limits work • Vitality: Degree of energy patients have • 6 minutes walk remained low • Only 49% had returned to work NEJM 2003: 348: 683-693
Summary • ARDS is a clinical syndrome characterized by severe, acute lung injury, inflammation and scarring • Significant cause of ICU admissions, mortality and morbidity • Caused by either direct or indirect lung injury • Mechanical ventilation with low tidal volumes and plateau pressures improves outcomes • So far, no pharmacologic therapies have demonstrated mortality benefit • Ongoing large, multi-center randomized controlled trials are helping us better understand optimal management
References Rubenfeld GD, et al. Incidence and outcomes of acute lung injury N Engl J Med. 2005;353:1685-93. Luhr OR, et al. Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. The ARF study group. Am J Respir Crit Care Med. 1999;159:1849061, Bersten AD et al. Australian and New Zealand Intensive Care Society Clinical Trials Group. Incidence and mortality of acute lung injury and the acute respiratory distress syndrome in three Australian states. Am J Respir Crit Care Med. 2002;165:443-8. Connors AF Jr, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT investigators. JAMA. 1996;276:889-97. Richard C, et al. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2003;290:2713-20. Wheeler AP, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med. 2006:354:2213-24. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301-8. National Heart, Lung and Blood Institues Acute Respiratory Distress (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N Enlg J Med. 2006;354:2564-75. Kollef, MH, Schuster DP. The acute respiratory distress syndrome. N Engl J Medicine 1995;332(1):27-37.
References Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2000;283:1995-2002. Anzueto A, et al. Aerosolized surfactant in adults with sepsis-induced acute respiratory distress syndrome. Exosurf Acute Respiratory Distress Syndrome Sepsis Study Group. N Engl J Med. 1996;334:1417-21. Dellinger RP et al. Effects of inhaled nitric oxide in patients with acute respiratory distress syndrome: results of randomized phase II trial. Inhaled Nitric Oxide in ARDS Study Group. Crit Care Med. 1998;26:15-23. Zapol WM, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA 1979;242:2193-6. Derdak S, et al. High-frequency oscillatory ventilation for adult respiratory distress syndrome: a randomized controlled trial. Am J Respir Crit Care Med. 2002;166:801-8. Bernard GR, et al. High-dose steroids in patients with the adult respiratory distress syndrome. N Engl J Med. 1987;317:1565-70. Steinberg KP, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006:354:1671-84. Ware LB, MA Matthay. The acute respiratory distress syndrome. N Engl J Med 2000;342:1334-49. Meduri GU et al. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA 1998;280:159-65. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med 2006;354:1671-84.