Download
1 / 25
250 likes | 404 Views
Abnormalities of the Conduction System Elizabeth Dugan - edugan@hmc.psu.edu Olamide Odubogun - oodubogun@hmc.psu.edu. Rhythm Of The Heart. The Heart is Like an Orchestra. It has a conducting system that is directed by a conductor. This conductor is the “Natural Pacemaker” of the Heart

E N D
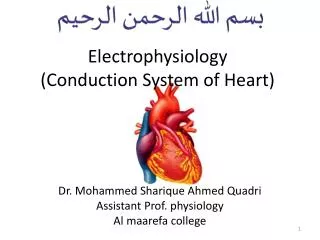
Abnormalities of the Conduction System Elizabeth Dugan - edugan@hmc.psu.edu Olamide Odubogun - oodubogun@hmc.psu.edu
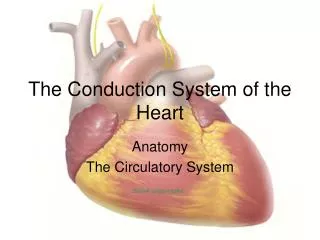
Rhythm Of The Heart • The Heart is Like an Orchestra. • It has a conducting system that is directed by a conductor. • This conductor is the “Natural Pacemaker” of the Heart • Conducting System: • SA node (Primary Pacemaker) • AV node • Bundle of His • Purkinje Fibers
Conducting System • Sino-Atrial node (SA Node) • -Origination and dissemination of electrical signals to BOTH atria • -Causes BOTH atria to contract • Atrioventricular Node (AV Node) • -Transmits signal to ventricles by going through interventricular septum • -Causes intentional delay, to allow atria to complete pumping • His Purkinje System • -Electrical signal flows through the His-Purkinje system and causes the ventricles to contract SIMULTANEOUSLY
Electrical Signal SA node fires electrical signal spreads through the Right and left atria Right and Left atria contract (blood moves from atria to ventricles) AV Node fires electrical signal spreads through His-Purkinje System Right & Left Ventricles Contract (blood moves from ventricles into aorta and pulmonary a.)
EKG Mechanics • WHAT does an EKG measure? • Measures electrical signals from heart. • This consists of: • Atrial contraction - P Wave • Ventricular contraction – QRS complex • Ventricular Relaxation – T Wave • HOLD ON!!!!! • What about Atrial Relaxation? • HOW does it do this? • Your body is a conductor of electricity • The electrical signal generated in the heart is • detected by the leads placed on the surface • of the body
Main EKG Waves Ventricles contract QRS complex Atria contract P Wave Ventricles Relax T Wave
Normal EKG P P P T T P T P T QRS QRS QRS QRS • Normal EKG: • Regular Rate –heart rate of 60-100 bpm • Regular Rhythm – P – QRS – T – P – QRS – T – P – QRS – T - etc • The height of the wave – related to the mass of the muscle generating the wave • - the ventricles have more mass than the atria: • - large ventricles (ventricular hypertrophy) more muscle creating a stronger signal when the ventricles contract: P wave is smaller than QRS complex taller QRS complex
Ventricular Hypertrophy (Large Ventricle) NOTICE the very large QRS complex in the EKG • Causes of a Large QRS Complex • Increased mass in: • One ventricle • Both ventricles • Portion of the ventricle QRS Normal EKG
ARRHYTHMIA Ventricular Fibrillation • Ventricular Fibrillation – disordered electrical activity • The ventricles "flutter" rather than beat and pump little or no blood. • In minutes, collapse and sudden cardiac death will follow • Medical help is needed immediately • Treatment - defibrillator
Hypertrophic Cardiomyopathy -Disease of the myocardium -Portion of the myocardium is thickened (hypertrophied, aka, the opposite of atrophy) -Individual muscle fibers are disorganized abnormal conduction + arrhythmias Hypertrophy is asymmetric The interventricular septum (muscle b/w the 2 ventricles) is usually enlarged much more than the rest of the ventricle
The ventricle is hypertrophied What happens to the following: Relaxation? Filling? Pressure? Forward Flow? What does all this cause? ALL ARE DECREASED! • Difficulty breathing!
Outflow tract obstruction – (the outflow tract is the path from the LV into the aorta) Outflow Obstruction Increased velocity!
Normal Flow Normal Velocity, Low Pressure Outflow Obstruction Fast Velocity, High Pressure When flow is obstructed, you need to build more muscle so that you can pump harder! This equals hypertrophy!
Mitral Regurgitation • Narrowed outflow tract = faster flow • Faster flow of blood pulls the mitral valve open • Blood goes back into the atria from the ventricle during systole mitral regurgitation Aortic Valve Regurgitation Mitral Valve Left Ventricle SHOW VIDEO HOW WE FIX MITRAL REGURG?
HCM Symptoms • Average age presentation : mid 20s • Wide range symptoms/severity • Difficulty breathing(dyspnea) • WHY? • Angina • WHAT DOES ANGINA MEAN? • Syncope (fainting) • FROM WHAT? • WHY WOULD FAINTING BE BENEFICIAL?
Interesting Facts • What is the most common cause of cardiac death in athletes? • Hypertrophic Cardiomyopathy • How many people does this affect? • 1/500 • Is everyone at risk for this? • Inherited (genetic) disorder: autosomal dominant, know your genetics and be careful if you are a possible carrier! • Does everyone with HCM have the same symptoms and outlook? • There are different forms of the disease and some are more severe than others incomplete penetrance
Physical Exam • Often are normal • Extra heart sounds • Fourth heart sound – this is heard before the “Lub” instead of “lub-dub” you here “da-lub-dub” • Systolic Murmur • Due to Turbulent (noisy) flow through the outflow tract (LV to Aorta) • Systolic Murmur • Due to regurgitation of blood through the mitral valve
HCM and Arrhythmias HCM: Disarray! Physiology 101: Structure = Function Thus, Abnormal Structure=… Normal Myocardium : Linear arrangement Where does most of the cardiac muscle increase? Interventricular Septum (IVS) What other structures did we mention in the last lecture were in the IVS? Thus, what could disarray in the IVS cause?
MYOCARDIAL DISARRAY • During Vfib • The ventricles are like bowl of jelly • - Inefficient pump • -Muscle cells malaligned • “Myocardial Disarray”
HHOW DO YOU SOLVE THIS PROBLEM?? Defribillators e.g. ICD 2) Pacemakers (artificial)
Implantable Cardioverter Defibrillator (ICD) An ICD is used in patients at risk for: 1. Ventricular tachycardia (>100 bpm) 2. Ventricular fibrillation 3. Sudden cardiac death caused by arrhythmias An ICD is made up of two parts: 1. Pulse generator – battery plus circuits 2. One or two leads (wires) How the ICD Works: 1. Leads monitor your heart rate 2. ventricular tachycardia or fibrillation detected controlled burst of impulses (called "overdrive" pacing) 3. If that does not work, the ICD "shocks" the heart to restore a normal rhythm. Newer ICD devices can also work like a pacemaker if a slow heart rate (bradycardia) occurs.
Pacemaker • Pacemakers are used to treat: • Abnormal rates • Bradycardia/ Tachycardia • Abnormal rhythms • Arrhythmia • Atrial fibrillation • Goals: • Coordinate the electrical signaling between the upper and lower chambers of the heart • Coordinate the electrical signaling between the ventricles An ICD is like a pacemaker in some ways, but it can use higher energy electrical pulses to treat certain dangerous types of arrhythmia.