Download

1 / 17

E N D
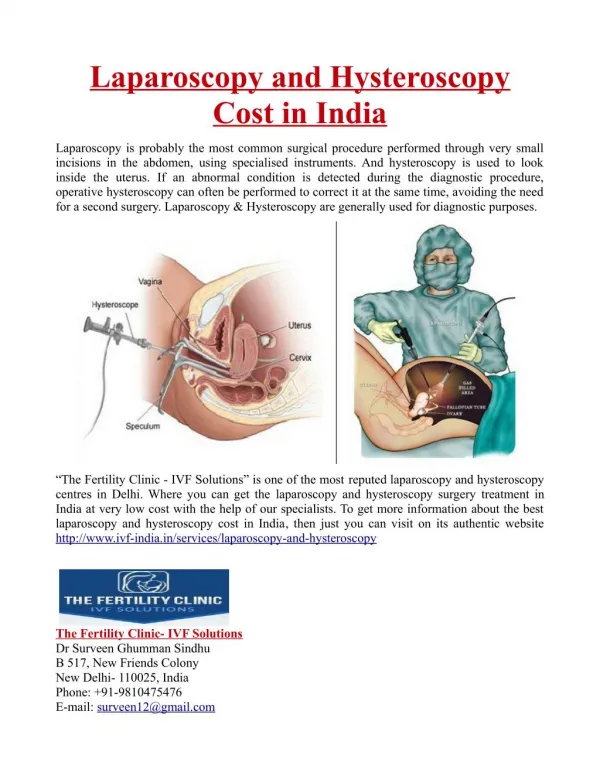
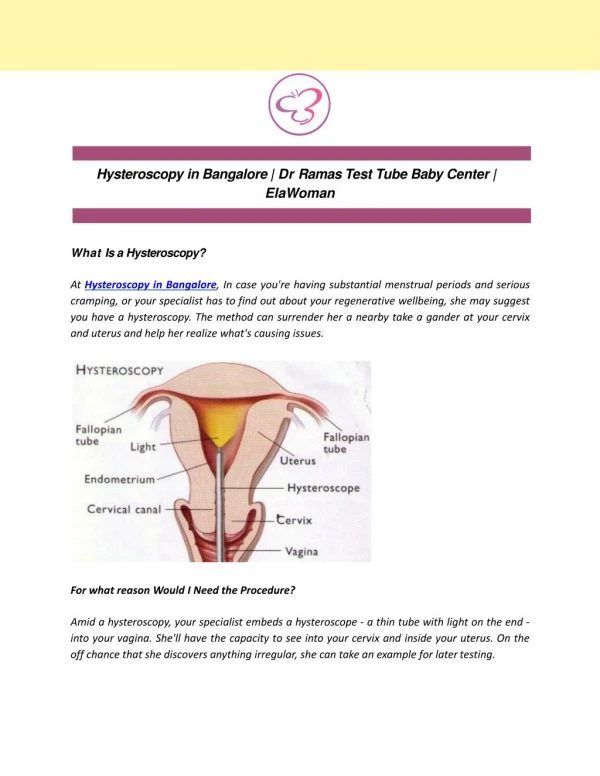
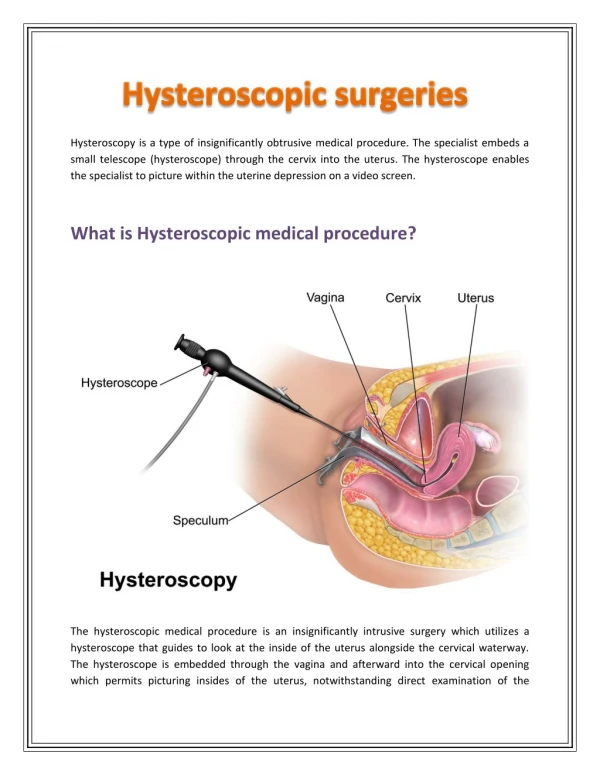
Diagnostic Hysteroscopy • Hysteroscopy is an important tool on the study of infertility, recurrent miscarriage, or abnormal uterine bleeding. Diagnostic hysteroscopy is used to examine the inside of the uterus, also known as the uterine cavity, and is helpful in diagnosing abnormal uterine conditions such as internal fibroids, scarring, polyps, and congenital malformations. A hysterosalpingogram (an x-ray of the uterus and fallopian tubes) or an endometrial biopsy may be performed before or after diagnostic hysteroscopy. • The first step of diagnostic hysteroscopy involves slightly stretching the canal of the cervix with a series of dilatators. Once the cervix is dilated, the hysteroscope, a narrow lighted viewing instrument similar to but smaller than the laparoscope, is inserted through the cervix and into the lower end of the uterus. Carbon dioxide gas or special clear solutions are then injected into the uterus through the hysteroscope. This gas or solution expands the uterine cavity, clears blood and mucus away, and enables the physician to directly view the internal structure of the uterus.
Diagnostic Hysteroscopy • Diagnostic hysteroscopy is usually conducted on an outpatient basis with either general or local anesthesia. Diagnostic hysteroscopy is usually performed soon after menstruation because the uterine cavity is more easily evaluated and there is no risk of interrupting pregnancy.
Distension Media • Carbon Dioxide • For diagnostic hysteroscopy, gaseous distension media are usually preferred. A continuous flow is necessary to replace gas lost through the tubes, around the hysteroscope and absorbed into the uterus. • High-viscosity Fluids • Dextran 70 has a molecular weight of 70000 and is a mixture of 32% dextran in 10% dextrose. It is a thick viscous fluid and is electrolyte free, non-conductive and biodegradable. • Low-viscosity Fluids • 5% DEXTROSE IN WATER • As this substance has no clinical advantages over 0.9% sodium chloride solution, but has this significant additional risk of dilutional electrolyte disturbance its use can no longer be recommended. • 1.5% GLYCINE • It is optically clear and non-hemolytic and does not conduct electricity. Excessive absorption of such an electrolyte-free solution can be associated with hyponatremia and hemolysis. • SORBITOL • It is optically clear and is being used as an alternative to glycine. • 0.9% SODIUM CHLORIDE • Normal saline is optically clear, cheap and readily available. Excess intravasation is not associated with any major electrolyte or metabolic disturbances and any fluid overload can be rapidly reversed with diuretic therapy alone.
Indications • Direct hysteroscopic inspection with adequate distention and visualization discloses almost every intrauterine abnormality with high accuracy. Additionally, it enables exact localization of the pathology and determination of its intracavitary extent. However, for the diagnosis of endometritis and adenomyosis, conclusive hysteroscopic criteria are still lacking.
Abnormal Uterine Bleeding • Abnormal uterine bleeding is the most common complaint of patients consulting the gynecologist and provides the most frequent indication for hysterectomy • Figure Endometrial polyp with atypical vessel structure.
Abnormal Uterine Bleeding For histologic examination selective samples of any abnormal tissue can be obtained by visually controlled biopsies. Figure Adenocarcinoma of the endometrium with an irregular surface with necrosis and dilated tortuous vessels.
Infertility • Hysteroscopic diagnosis and treatment appear to have been very important in patients with infertility or recurrent pregnancy loss. The method should be considered as complementary to TVS and HSG rather than competing with them in these patients. • Diagnostic hysteroscopy is always needed for intrauterine filling defects on HSG to confirm or exclude pathology and to determine the nature of an abnormality and the possibilities for transcervical endosurgical treatment. • FigureHSG with intrauterine filling defects caused by grade III IUAs
Intrauterine Adhesions • If the filling defects are caused by intrauterine adhesions, for which treatment by hysteroscopy is the method of choice, any other 'blind' intrauterine procedure can deteriorate the possibilities for hysteroscopic treatment by creating a false route or perforation and reducing the amount of residual normal endometrium, which is required for adequate regeneration after synechiolysis. • Figure Grade III IUAs
Submucous Myomas • Submucous myomas can be a reason for infertility or pregnancy loss. They generally cause abnormal uterine bleeding, but may be asymptomatic and only present as intracavitary filling defects during HSG in infertility patients. In these cases hysteroscopic diagnosis will disclose the nature and extent of the pathology and the possibilities for endosurgical treatment
Others • Other intrauterine disorders that may interfere with fertility and cause bleeding abnormalities are endometrial polyps, endometrial hyperplasia and endometritis. • Specific indications for diagnostic hysteroscopy in infertility patients are: • Abnormal uterine bleeding. • History of complicated intrauterine procedures or uterine surgery. • History of recurrent pregnancy loss. • Intrauterine abnormalities on TVS. • Abnormalities of the uterine cavity or intrauterine filling defects with HSG. • Together with laparoscopy if no hysteroscopy has been performed before. • Infertility with unknown cause. • Unsuccessful in vitro fertilization and embryo transfer (IVF-ET) if no hysteroscopy has been performed before.
Other Indications • SECONDARY DYSMENORRHEA • As secondary dysmenorrhea often appears to be due to intrauterine disorders such as submucous myomas, endometrial polyps or IUAs, hysteroscopic diagnosis should be performed in these cases as first diagnostic method. • 'MISSING' INTRAUTERINE CONTRACEPTIVE DEVICE (IUCD) • If the retrieval threads of an IUCD are not visible, its location can be determined by ultrasonography. Hysteroscopy is the method to remove the IUCD safely under direct visual control.
Minor Intrauterine Procedures • In a significant number of cases minor intrauterine diagnostic or therapeutic interventions can be performed during a diagnostic procedure, for example: • Biopsies. • Polypectomy. • Synechiolysis. • Focal coagulation.
Operative Hysteroscopy • Operative hysteroscopy can treat many of the abnormalities found during diagnostic hysteroscopy. Operative hysteroscopy is similar to diagnostic hysteroscopy except that a ideal hysteroscope is used to allow operating instruments such as scissors, biopsy forceps, electosurgical or laser instruments, and graspers to be placed into the uterine cavity through a channel in the operative hysteroscope. Fibroids, scar tissue, and polyps can be removed from inside the uterus. Congenital abnormalities, such as uterine septum, may also be corrected through the hysteroscope.
Operative Hysteroscopy • After surgical repair of the uterine cavity, a Foley catheter or intrauterine device (IUD) may be placed inside the uterus to prevent the uterine walls from fusing together and forming scar tissue. Antibiotic and/or hormonal medication may also be prescribed after uterine surgery to prevent infection and stimulate healing of the endometrium (uterine lining). Endometrial ablation, an operative hysteroscopy procedure in which the endometrium is destroyed, can be used to treat excessive uterine bleeding when a hysterectomy is not considered feasible.
Risks of Hysteroscopy • Complications of diagnostic hysteroscopy are rare and seldom life-threatening. Perforation of the uterus is the most common, When operative hysteroscopy is planned, diagnostic hysteroscopy is frequently performed at the same time to allow the physician to see the outside as well as the inside of the uterus. • Complications occur in one or two out of every 100 operative hysteroscopy procedures, with uterine perforation being the most common. Some complications related to the liquids used to distend the uterus include pulmonary edema (fluid in the lungs), breathing difficulties, blood clotting problems, decreased body temperature, and severe allergic reactions. Complications related to the surgical procedure include damage to intra-abdominal organs and hemorrhage.
Conclusion • Diagnosing and correcting gynecologic disorders once required major surgery and many days of hospitalization. Laparoscopy and hysteroscopy now allow physicians to diagnose and correct many of these disorders on an outpatient basis. Patient recovery time is normally only two to three days, which is significantly less than the recovery time from major abdominal surgery. The procedures also decrease patient discomfort. Before undergoing laparoscopy or hysteroscopy, patients should discuss with their physicians any concerns about the procedures and their risks.