Download
1 / 35
350 likes | 825 Views
UTERINE CAVITY FINDINGS BY HYSTEROSCOPY IN IVF FAILURE. Assoc. Prof. Dr. Rafael LEVİ Ege University Family Planning And Infertility Research And Treatment Center-İZMİR 2. Güncel Üreme Endokrinolojisi, Yardımcı Üreme Teknikleri Kongresi 1. Üreme Tıbbı Derneği Kongresi

E N D
UTERINE CAVITY FINDINGS BY HYSTEROSCOPY IN IVF FAILURE Assoc. Prof. Dr. Rafael LEVİ Ege University Family Planning And Infertility Research And Treatment Center-İZMİR 2. Güncel Üreme Endokrinolojisi, Yardımcı Üreme Teknikleri Kongresi 1. Üreme Tıbbı Derneği Kongresi 17-20 Nisan 2008 Çeşme- İzmir
Investigation and current management of recurrent IVF treatment failure in the UK.Tan BK et all, BJOG, 112(6):773-80 2005 Objective: To determine current practice in the management of recurrent IVF treatment failure in licenced UK infertility centers. • Human Fertilization And Embriyology Authority licenced centers in UK (n=79) • How recurrent IVF treatment failure was defined? Which investigations were initiated? Which therapeutic options were subsuquently recommended? RESULTS: • The most common definition was three unseccessful IVF cycles (range 2-6) • Anticardiolipin antibodies and lupus anticoagulan antibodies • Hysteroscopy • Karyotype • Blastocyst culture • Assisted Hatching The results of this survey suggest that there is considerable variation in the approach to investigation and management of recurrent IVF treatment failure in the UK.
Definition of Repeated Implantation Failure • Failure to achieve a pregnancy following 2-6 IVF cycles, in which more than 10 high-grade embryos were transferred to the uterus was defined by various clinicians as ‘repeated implantation failure’. Tan et all, 2005 • Today with the tendency of transferring only one or two embryos, the definition of repeated implantation failure is not apparent. After failure of two or three cycles in which reasonably good embryos were transferred further investigation should be initiated. Margolioth EJ et all, 2006
Shamma FN et all, Fertil Steril, 1992Balmaceda JP, Obstet and Gynecol Clinicf of North America , 1995 The major determinant of the success of IVF treatment is embryo quality. Uterine receptivity and uterine integrity have also an important impact for the achievement and continuation of pregnancy. It has been well established that implantation of fertilized eggs is affected by intrauterine environment.
Margalioth EJ et all, Hum Rerod 21(12):3036-43, 2006 The causes for repeated implantation failure may be because of embrionic defects, reduced endometrial receptivity or multifactorial effects. Various uterine abnormalities, thin endometrium, altered expression of adesive molecules and immunological factors may decrease endometrial receptivity. Genetic abnormalities of the male or female, sperm deffects, embrionic aneuploidy, zona hardening are among the embrionic reasons for failure of implantation. Endometriosis and hydrosalpinges may adversely influence both.
The Uterine Abnormalities In Infertile Women • Uterine malformations • Myomas • Endometrial polyps • Intrauterine adhesions • Endometritis • Thin endrometrium • Endometrial Hyperplasia • Cervical adhesions Lass A et all, Journal of Assisted Reproduction And Genetics, 16, 410-15,1999 Varasteh NN et all, Obstet Gynecol 94, 168-171, 1999
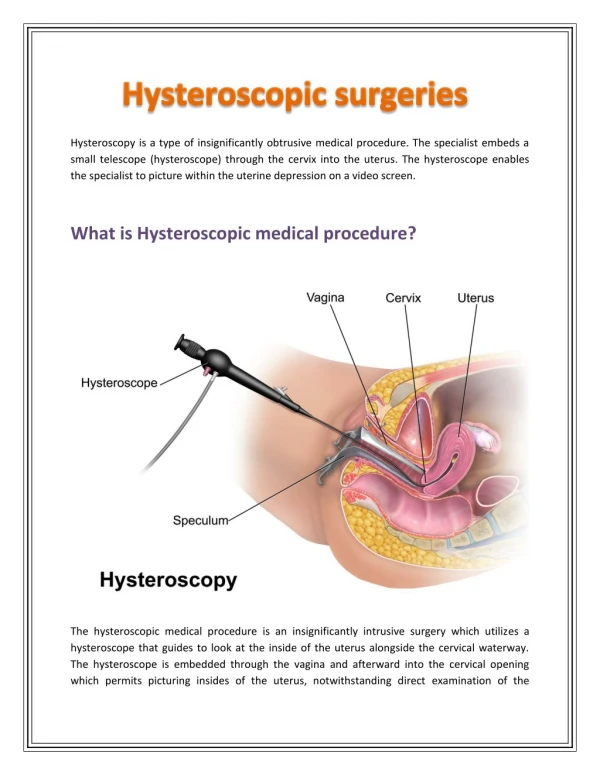
To diagnose intrauterine pathologies in infertil women: • Transvaginal ultrasonography • Saline infusion sonography • Hysterosalpingography • Hysteroscopy
Hysteroscopy is superior to hysterosalpingography for diagnosis of intrauterine pathology and it is not suprising that anomalies might be overlooked when relying on HSG alone. Golan A et all, Acta Obstetrica et Gynecologyca Scandinavia, 75,654-56-1996 • Hysteroscopy demonstrates not only the location, shape and size of adhesions, but also their nature ( mucosal, fibrous, myometrial). Al-Inany H. Acte Obstetrica et Gynecologyca Scandinavia, 80, 986-93, 2001
Sonographic findings of 879 infertile patients. Sensitivity of USG 20% Specificity of USG 95% Positive predictive value 64% Negative predictive value 74% Ege University IVF Center
Hysterosalpingographyc findings of 585 infertile patients. Sensitivity of HSG 85% Specificity of HSG 56% Positive predictive value 46% Negative predictive value 89% Ege University IVF Center
Hysteroscopic findings of 879 infertile patients. Ege University IVF Center
Hysteroscopic findings of 98 patients who had 2 unsuccessful IVF cycles. Ege University IVF Center
Hysteroscopy in on IVF-ET programme. Clinicial experience with 360 infertile patients.Senera P et all, Acte Obstet Gynecol Scand 67(2): 135-137,1988 360 patients underwent hysteroscopy before entering the IVF program (247-%70- was obstructive tubal disease). • 148 showed uterine abnormalities (44,5%) • Endometrial polyps • Adhesions • Hypoplasie • Malforrnations • Cervical stenosis • 114 of these patients had normal hysterographic findings. In an IVF programme hysteroscopic evaluation can reduce the failure rate due to intrauterine abnormalities.
The role of hysteroscopy in patients having failed IVF/GIFT transfer cycles.Kirsop R. et all, Aust NZJ Obstet Gynecol 31(3):263-4,1991 • 50 patients who had undergone 2 or more failed IVF cycles or failed GIFT cycles. • Fertilization have been demostrated. Hysteroscopy RESULTS: 28 % were found to have intrauterine abnormalities. Patients with an abnormality found at hysteroscopy had undergone a significantly higher mean number of transfer cycles. These results suggest that intrauterine abnormalities may be cause for failure of IVF-ET or GIFT. Hysteroscopy should be part of the infertility work-up of all patients prior to undergoing IVF treatment.
The role of diagnostic hysteroscopy and endometrial, biopsy in ART La Sala GB et all,Fertil Steril, 70(2), 378-80,1998 Objective: To study the medicine of unsuspected endouterine abnormalities in patients for whom IVF-ET repeatedly fails • 100 patients • 2 IVF cycles failed (2≥good quality embryos) • RESULTS: In 18 patients hysteroscopy showed endouterine abnormality. • 6 endometrial polyps • 3 submucous myoma • 7 intrauterine adhesions • 1 endometritis • 1 tuberculous endrometritis Conclusion: Diagnostic hysteroscopy should be performed on all patients before they undergo IVF-ET.
The value of repeat hysteroscopic evaluation in patients with failed IVF transfer cycles.Dicker D et all, 58(4):833-5, Fertil Steril, 1992 • 110 women with normal initial hysteroscopy • 3 or more repeated implantation failure with IVF. • RESULTS: 20 patients (18,2%) with uterine abnormalities. • Hyperplasia • Polyps • Endometritis • Synechiae • Our results indicate that repeat hysteroscopic evaluation in cases of recurrent IVF-ET failure is an important adjunctive method for further avaluating and posibly optimizing the IVF-ET procedure.
The value of hysteroscopy after repeated implantation failures with IVFSciano A et all. Contracept Fertil sex 27(2):129-132,1999 Objective: To determine the usefulness of uterine re-assessment by hysteroscopy in women with 2 unsuccessful IVF-ET. • 73 infertile women • Repeat hysteroscopy after 2 implantation failure in IVF RESULTS: 50% of the cases an abnormality was diagnosed. • Cervical synechiae polyp false passage • Hormono-dependent abnormalities polyp hyperplasia submucous myoma • 22% of these patients →pregnant It seems legitimate to perform hysteroscopy in women who have had 2 IVF-ET failure before attempting a third procedure.
Effect of treatment of intrauterine pathologies with office histeroscopy inpatients with recurrent IVF failureDemirol A, Gürgan T, Reprod Biomed Online 8(5): 590-42004 Objective: The study was conducted to evaluate if the diagnosis and treatment of intrauterine lesions with office hysteroscopy is of value in improving the pregnancy outcome in patients with recurrent IVF failure. • 421 patients who had undergone 2 or more falled IVF cycles (prospectively randomized) Group I: (n=211) did not have office hysteroscopic evaluation Group II: (n=210) had office hysteroscopy Group IIa: (n=154) normal hysteroscopic findings Group IIb: (n=56) abnormal hysteroscopic findings(corrected at the same time ) • No difference existed in the mean number of oocyte retrived, fertilization rate, number of embrios transferred or first trimester abortion rates among the groups.
Effect of treatment of intrauterine pathologies with office histeroscopy inpatients with recurrent IVF failureDemirol A, Gürgan T, Reprod Biomed Online 8(5): 590-42004 Results: Clinicial pregnancy rates: Group I: 21,6% Group IIa: 32,5% p=0,044 Group IIb: 30,4% p=0,044 Patients with normal hysterosalpingography but recurrent IVF failure should be evaluated by hysteroscopy.
Objective: To evaluate if the diagnosis and treatment of the uterine cavity abnormalities by hysteroscopy in IVF is of any value in improving clinical pregnancy outcome • 520 patients who had undergone 2 or more falled IVF cycle • Group I(n=265) without office hysteroscopy Group II(n=255) had office hysteroscopy Group II a (n=160)had normal findings Group IIb (n=95) had abnormal findings (corrected at the same time) • No difference in the mean number of oocytes retrieved, fertilization rate, number of embryos transferred Rama-Raju GA et al., Archieves of Gynocology and Obstetrics 274(3):460-462, 2006
Result: clinical pregnancy rates Group I 26,2 % Group IIa 44,44 % (p<0,05) Group IIb 39,55 % (p<0,05) • Patients with recurrent IVF failure after normal HSG should also be reevaluated using hysteroscopy Rama-Raju GA et al., Archieves of Gynocology and Obstetrics 274(3):460-462, 2006
The value of hysteroscopy in elderly women prior to IVF-ET: a comparative study Dicker D.et al., J In Vitro Fert Embryo Transf. 1990 • 284 hysteroscopies were performed in 312(91%) candidates for IVF who were divided into 2 groups; • Group I; elderly women over 40 years (n=66) • Group II; below 40 years (n=218) • All of which failed in 1 to 3 cycles previously • Results; Uterine abnormalities in all patients 29,9% Abnormal findings were significantly increased in group I (p<0,001)
The value of hysteroscopy in elderly women prior to IVF-ET: a comparative study Dicker D.et al., J In Vitro Fert Embryo Transf. 1990 • In elderly women age related uterine pathology such as submucos myoma, endometrial hyperplasia and polips were more prominent. In younger patients adhesions and tubal ostia occlusion were more common. • 7 clinical pregnancies (8,9%) in Group I • 41 clinical pregnancies (19,9%) in Group II (treatment prior to IVF) • All of which failed in one or three cycles previously • It seems that hysteroscopic evaluation may reduce the IVF-ET failure rate due to intrauterine abnormalities in elderly as well as young patients
The Association Between Uterine Septum and Infertility Abuzeid M. Et al. Fertil Steril, 2005 • Objective: To report the incidence of short uterine septum in infertility patients based on hysteroscopic findings • 1011 patients who underwent laparoscopic and hysteroscopic surgery for treatment of infertility Group I: 661 patients with endometriosis Group II: 350 patients who had no endometriosis • If a uterine septum was detected the type was determined : short <2cm long>2 cm • Hysteroscopic division was performed • Following surgery 33 patients underwent ART
Results; The mean age of the women with septum 31,0±5,1 Duration of infertility, 3,6 ±3,4 years Uterine septum in Group I 117( 17,7%) in Group II 61 (17,4%) Short type in Group I 15,6 % in Group II 14,3 % • 33 patients who attended ART pregnancy rate 51,9% Conclusion; The incidence of short uterine septum in infertile patients is much higher than what has previously been reported After hysteroscopic surgical correction high pregnancy rates can be achieved after assisted conception Abuzeid M. Et al. Fertil Steril, 2005
Is hysteroscopic correction of an incomplete uterine septum justified prior to IVF Özgür K et al. Reprod Biomed Online 2007 • Objective: To examine the effect of hystreroscopic correction of an incomplete uterine septum on IVF outcome • Mesurement of fundal myometrial thicness (Fm) cornual myometrial thicness (Cm) By sonohysteroscopy • Incomplete septum criteria: Fm> 11 mm and Fm-Cm> 5 mm • Group I ( n=119) patients with incomplete septum • Grup II (n=116) control patients; age matched with normal cavity who underwent IVF with in the same time period • Result: Group I had a hystory of more spontaneus abortions (14,20 vs 6,03 % p=0,04) • Group I higher previous IVF failure (32,7 vs 20,6 % p=0,04) • After surgical correction of the septum in Group I; IVF pregnancy outcome was similar in both groups clinical pregnancy rates 47,8% vs 46,5% pregnancy loss 10,52% vs 20,3%
Hysteroscopic findings in women with a history of very thin endometrium during assisted conception treatment:Marikinti K. Fertil Steril 84(1); 364-65, 2005 • Objective: To study the value of hysteroscopy in ‘thin endometrium’ on transvaginal sonography • A thin endometrium on transvaginal sonography is the most vidaly used screening test for endometrial inadequency • 34 women with thin endometrium (≤6 mm prior to embryo transfer) underwent both a repeat TV sonography and hysteroscopy either during and abondoned treatment cycle or in a naturalş cycle after the failed attempt • Results: All 34 cases gave a hystory of uterine interventions : 18 uterine evacuations 8 assisted conception related procedures 3 caesarean sections 2 endometritis 2 peritonitis 2 myomectomy
The hysteroscopic findings:Group A (n=14): narrow glandular openings, thin blood vessels mal distributed, fragile Em. 8 samples out of phase em, 13 non homogeneus and/or non trilaminar em Group B (n=12): moderately developed glandular openings, blood vessels uniformly distributed, healthy Em, 1 sample out of phase Group C (n=8): Intra uterine synechie, obliteration of the uterine cavity. 3 samples out of phase Em. 4 non homogeneus and/or non trilaminer Em 34 womens subsequently underwent 6 cycles of high dose estrogen therapy, aspirin or empirical antibiotics Follow-up TV sonography; 21 cases: 7,2 mm endometrial thicness 13 cases: ≤ 6 mm endometrial thicness Group A (6/14) attempted to conceive following hysteroscopy 2 singleton livebirth Group B (11/12)1 singleton livebirth Group C (4/8)1 singleton livebirth 4 pregnancies were complicated by recurrent bleeding and preterm delivery and 1 required a caesarean hysterectomy for placenta accreata Marikinti K. Fertil Steril 84(1); 364-65, 2005
Hysteroscopic findings in women with a history of very thin endometrium during assisted conception treatment:Marikinti K. Fertil Steril 84(1); 364-65, 2005 • Conclusion: • The hysteroscopic findings of atrophic Em, correlated well with poor grade Em on trans vaginal USG and out of phase histology which may have led to the low uptake of further treatments. • The presence of thin but healthy Em at hysteroscopy correlated well with a good grade of Em on TV-USG and in phase histology, which probably led to the high uptake rate of further treatments. But the pregnancy rate remained low. • In group C, selected cases of treatable Asherman’s Syndrome achieved pregnancies that were high risk .
Chromo-hysteroscopy for evaluation of endometrium in recurrent IVF failure Küçük T, Safali MAssit Reprod Genet 25(2-3); 79-82, 2008 • Objective: To assess the efficacy of chromo-hysteroscopy in detecting endometrial pathologies in recurrent IVF failure • 64 patients in whom conventional hysteroscopy did not show any apparent endometrial pathology. • 5 ml. of 1 %methylene blue dye was introduced through the hysteroscopıc inlet. • Biopsies were obtained both from dark stained and light stained areas. • Group I :22 patients with focal dark staining • Group II:41 patients with light blue staining • No significant difference between two groups in age,smoking,BMI,number of IVF failure.
Result: There was a statistically significant difference in the incidance of endometritis between two groups (p=0,007) • The power of dark staining for detection of endometritis was calculated as follows: sensitivity 69,2 % specificity 74 % positive predictive value 40,9 % negative predictive value 90,2 % • Chromo-hysteroscopy improves the efficacy of hysteroscopy in recurrent IVF failure. Küçük T, Safali M Assit Reprod Genet 25(2-3); 79-82, 2008
Polypoid appearance of the endometrium on office hysteroscopy a significant predictor of miscarriage after IVF-ETZeyneloglu HB et al., Fertil Steril 2007 • Objective: To assess the impact of polypoid appearance detected by office hysteroscopy on clinical pregnancy and abortion rates in IVF cycles • Patients in whom office hysteroscopy was performed in between days 17-20 of their menstruel cycle prior to their IVF-ET • Polypoid structures were biopsied using grasper or scissors or pipelle • Group I: (n=41) polipoid endometrium • Group II: (n=48) no abnormalities
No statistically significant differences in between the groups with respect to age, basal FSH levels, basal E2 levels, BAF count, BMI, the number of embryos transferred and causes of infertility Results: implantation rates Group I 69% Group II 52% p=0,43 (NS) abortion rates Group I 25,6% Group II 6,5 % p=0,01 Conclusion: A polypoid appearance of the endometrium may negatively affect the IVF result by increasing the abortion rates rather than directly influencing the pregnancy rates. Zeyneloglu HB et al., Fertil Steril 2007
Pregnancy rates after hysteroscopic polypectomy and myomectomy in infertile women.Varasteh NN, Neuwirth RS et al., Obstet Gynecol, 1999 • 78 patients with bilateral tubal occlusion; 36 patients hysteroscopic myomectomy 23 patients hysteroscopic polypectomy 19 patients normal Following surgery 78 patients underwent ART No significant difference in age, type of infertility and length of infertility • Results: Polypectomy subjects had significantly higher pregnancy and LBR than women with normal cavities (RR 2.42, p=0,06) • Women who had myomectomies larger than 2 cm. had significantly higher pregnancy and LBR, achieving statistical significance at a myoma size of ≥3 cm (3,15 cm versus 2,5 cm p=0,05) • Spontaneus abortion rates among first pregnancies after myomectomy, polypectomy or normal cases were similar • Both hysteroscopic polypectomy and hysteroscopic myomectomy appear to enhance fertility.
Conclusion • Hysteroscopy is the gold standard in infertile patients for determining uterine cavity and should be performed especially in women with ≥2 unsuccessful IVF cycles. • Repeat hysteroscopic evaluation in cases of recurrent IVF-ET failure is an important adjunctive method for further evaluating and possibly optimizing the IVF-ET procedure.