Download
1 / 36
400 likes | 1.72k Views
Varicella –Zoster Virus (VZV). Causes 2 major diseases Varicella (chicken pox): primary infection usually in childhood Zoster ( shingles): reactivation of an earlier varicella. Varicella (Chicken Pox). Mild, highly contagious disease chiefly affecting children Mode of transmission:

E N D
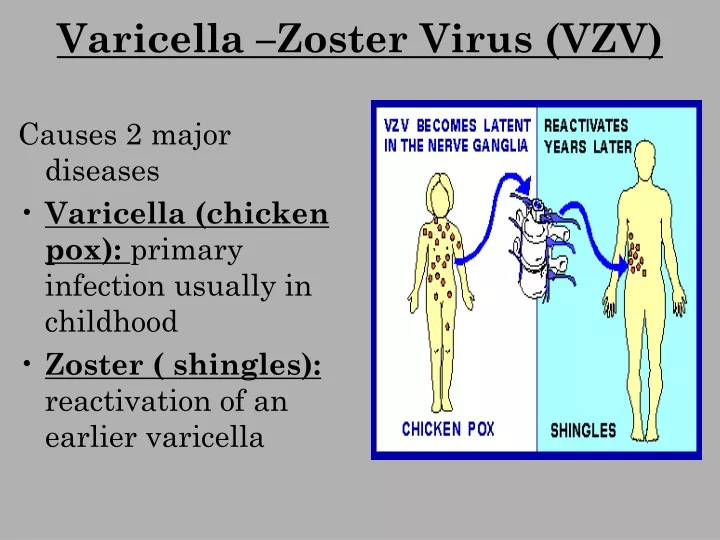
Varicella –Zoster Virus (VZV) Causes 2 major diseases Varicella (chicken pox): primary infection usually in childhood Zoster ( shingles): reactivation of an earlier varicella
Varicella (Chicken Pox) • Mild, highly contagious disease chiefly affecting children • Mode of transmission: - airborne droplets and direct contact from varicella patients - Vesicular fluid of Zoster patients can be the source of Varicella in susceptible children
Pathogenesis • VZV infects the mucosa of the upper respiratory tract • Multiplies in the regional LNs • Primary viremia and spread to liver and spleen • Secondary viremia follows with viral spread to the skin • Typical rash occurs • VZV remains latent in the dorsal root ganglia for life
Clinical Picture • Incubation period: 10-21 days • Symptoms: mild fever & rash • Rash: first appears on the trunk, then face but sparing distal parts of limbs (Centripetal distribution) • Flat macules become papules then vesicles • Followed by crust formation • The crust is often shed off and heals without scarring
Cropping is a characteristic feature of varicella rash: fresh vesicles appear in crops, so that all stages of macules, papules, vesicles & crusts are seen at the same time • More severe in adults: Hemorrhagic, bullous lesions, heal with scar
Complications 1- Pneumonia especially in adults, may be fatal 2- Rarely: fulminant encephalitis, which may be a manifestation of Reye’s syndrome that occurs as a consequence of salicylates intake during infection 3- Myocarditis, nephritis, acute cerebellar ataxia, meningitis and encephalitis
Congenital Varicella Syndrome & Neonatal Varicella • Primary maternal infection during the 1st trimester may lead to congenital varicella syndrome ( serious & fatal): skin lesions, hypoplasia of limbs, chorioretinitis & CNS defects • Primary maternal infection during last trimester can lead to widely disseminated infection in the new born with mortality rate of 35%. • If rash began a week or more before delivery, maternal Abs transferred via placenta – baby gets the infection but escapes clinical disease
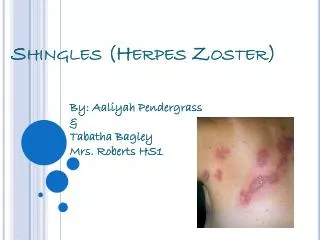
Zoster (shingles) • Sporadic disease in adults or immunocompromised patients • Results from reactivation of latent VZV • Rash similar to varicella but limited to a nerve distribution to the skin innervated by a dorsal root ganglion (dermatome)
Varicella-Zoster Virus (VZV) • Initial infection usually in childhood with Varicella virus (HHV-3): Chicken Pox • It is spread by respiratory aerosols or direct contact with lesions • The virus establishes latency within the dorsal root ganglia • Years or decades later, the virus (Herpes zoster) may reactivate -> Shingles
Varicella-Zoster Virus (VZV) Zoster means girdle, from the characteristic rash that forms a belt around the thorax Rash along dermatomes
VZV- Pathology Trigeminal nerve reactivation uveitis, keratitis, conjunctivitis Cranial nerve reactivation Bells palsy: a condition that causes the facial muscles to weaken or become paralyzed. It's caused by trauma to the 7th cranial nerve and is not permanent.
Ramsay-Hunt syndrome: • Virus spread to facial nerves. • Characterized by intense ear pain, a rash around the ear, mouth, face, neck, and scalp, and paralysis of facial nerves. • Symptoms may include hearing loss, vertigo, and tinnitus. Post-herpetic neuralgia: • chronic burning or itching pain; hyperesthesia (increased sensitivity to touch)
Laboratory Diagnosis • Specimen: Vesicular lesions smears 1- Direct Virus Demonstration: a) L/M: Tzanck smear – from the base of vesicles, 1% aq. soln. of toluidine blue ‘O’ shows multinucleated giant cells with faceted nuclei & homogenously stained ‘ground glass’ chromatin (Tzanck cells)
B) Direct Immunofluorescence: C) PCR: for detection of viral DNA 2- serology: Specific VZV Abs using CFT, Nt, or ELISA
Epstein- Barr virus • Ubiquitous human herpes virus. • By adulthood 90 to 95% of most populations are positive. • Spread occurs by intimate contact between susceptible individuals and asymptomatic shedders of EBV. • Mostly causes asymptomatic infections.
Transmission • Source: Oropharymgeal secretions/ saliva of infected persons. • Intimate oral contact, such a kissing leads to transmission (Kissing Disease). • May also follow blood or bone marrow transplants.
Pathogenesis Attaches to CR2 (CD 21) receptor (same as C3d complement receptor) Entry and multiplies locally Invades blood stream Infects B Lymphocytes Polyclonal activation Latency and immortalisation of B cells of B cells
Lytic Infection • The ZEBRA protein is expressed in epithelial cells • This transcription factor promotes the expression of early genes -> active virus replication and lytic infection Latency • B lymphocytes are only semi-permissive for replication and EBV infection is often latent • The infected B-lymphocyte contains a few episomes • Only a few genes are expressed from the episome, including two membrane proteins that are oncogenic • Burkitts lymphoma • Nasal pharyngeal carcinoma
Epstein Barr Virus (EBV) • In addition: • Infectious mononucleosis • Chronic fatigue syndrome
Infectious Mononucleosis (Glandular fever) • Acute self limited illness following primary infection with EB virus. • Incubation period is 4-8 weeks. • Fever, sore throat, lymphadenopathy, tonsillitis, enlarged spleen and liver • Occasional rash. • Ampicillin treated patients develop more rashes due to immune complex reactions. • The severity of disease often depends on age, but usually resolves in 1 to 4 weeks • In some Chronic fatigue (Mental and physical)
Laboratory diagnosis Peripheral blood smear: • Initially leucopenia • Prominent lymphocytosis • Abnormal mononuclear cells: Deeply basophilic & vacuolated cytoplasm, kidney shaped nuclei, lattice of fenestrated chromatin. • Not infected B cells • T cells reactive to virus infection.
Paul-Bunnell test • Standard diagnostic procedure • Heterophile agglutination test • Inactivated serum in doubling dilutions are mixed with equal volumes of 1% sheep erythrocytes • Incubate at 370 C for 4 hours • Examined for agglutination • Titre of 100 or above is suggestive of EBV • Confirmation: • Differential adsorption of agglutinins with guinea pig and Ox red cells
This test appears early in infection and disappears within two months
Other tests • IgM VCA (Virus capsid antigen) rises and disappears in 1-2 weeks: Reliable indicator for primary infection. • VCA IgG antibodies persist throughout life: Indicates past infection. • Appearance of Ab to EBNA (EB nuclear Ag): useful marker for primary infection
Cytomegalovirus (CMV) • Formerly known as salivary gland virus • Characterised by enlargement of infected cells and prominent intra-nuclear inclusions. • Prolonged latency in infected hosts • In neonate and immunodeficient: severe disease • Virus exhibits strict host specificity. • Human CMV is unrelated genetically with other herpes and even with CMV of other species.
Pathogenesis CMV (HHV-5) derives its name from the fact that it can form multinucleated cells (syncytia) Some cells such as macrophages and fibroblasts support a productive infection Other cells such as T lymphocytes and stromal cells of the bone marrow set up latent infection
Pathogenesis • The virus is spread via most secretions, particularly saliva, urine, vaginal secretions and semen • CMV may also be spread by blood transfusion and organ transplant • CMV causes no symptoms in children and mild disease in adults
Pathogenesis • Primary infection in older children and adults are asymptomatic. • Clinical infection is caused during to intrauterine or postnatal infections. • Intrauterine infection leads to fetal death or cytomegalic inclusion disease. • Cytomegalic inclusion disease is often fatal, associated with hepatosplenomegaly, jaundice, thrombocytopenic purpura & hemolytic anaemia. • Chorioretinitis, & cerebral calcification, mental retardation.
CMV • The virus elicits both humoral and cell-mediated immunity but the infection is not cleared • The virus may reactivate, particularly in cases of immuno-suppression • Organ transplant patients • Immunosuppressive disease • (CMV-retinitis occurs in up to 15% of all AIDS patients; also pneumonia, colitis, esophagitis and encephalitis)
Lab Diagnosis • Urine, saliva or other body fluids. • Human fibroblast cell cultures • Demonstration of cytomegalic cells in the centrifuged deposits from the saliva Owl’s eye appearance
Prevention • No licensed vaccine is available. • There is a candidate live attenuated vaccine known as the Towne strain125 and AD 169 strains. • But there are concerns about administering a live vaccine which could become latent and reactivate
Human Herpes virus 6 • Human B cell lymphotrophic virus • Ubiquitous and spreads through saliva in early infancy • Two variants A & B • Variant B causes Exanthem subitum (Roseola infantum or sixth disease)
Human Herpes virus 8 • Human Herpes virus 8 (HHV-8), or Kaposi Sarcoma Herpes Virus (KSHV), is associated with the development of Kaposi’s Sarcoma in AIDS patients. • Kaposi's sarcoma is a type of cancer that affects men and is rarely seen in women. • Although KS mainly affects the skin, the mouth, and the lymph nodes, it can also involve the bowels and lungs. • HHV 8 is sexually transmitted.