Download
1 / 36
390 likes | 558 Views
Learn about the basics of Primary Sclerosing Cholangitis (PSC), its etiology, clinical presentation, diagnosis, and prognosis. Discover key facts, epidemiology, and special considerations for variant forms of PSC.

E N D
Primary Sclerosing Cholangitis: The Basics Carlos J. Romero-Marrero MD MScChief of HepatologyDigestive Disease and Surgical Institute Cleveland Clinic
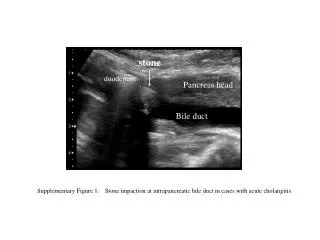
Case scenario • 32 y/o male presents with fatigue, pruritus, abdominal pain, diarrhea. Physical examination unremarkable except for abdominal discomfort. • ALT 43, AST 39, Alk Phosphatase 700, T bili 1.2, INR 1.0, albumin 4.2, AMA negative, ANA negative. Ultrasound shows mild diffuse intrahepatic biliary dilatation, no obvious masses.
Primary Sclerosing Cholangitis (PSC) • Is one of the cholestatic liver disorders • Cholestasis (“a standing still of bile”) is defined clinically as jaundice and/or itching and biochemically by varying degrees of elevation in alkaline phosphatase and bilirubin • Chronic cholestatic liver disease characterized by diffuse inflammation and fibrosis of both intra- and extra-hepatic bile ducts • May lead to liver cirrhosis, portal hypertension, and liver failure
Etiology and pathogenesis of PSC • Exact causes of PSC –unknown, however believed to be multifactorial • Data supporting genetic predisposition • Familial occurrence of PSC • Association of certain haplotypes (HLA chrom 6p21, HLA B*08, HLA-DRB1) with the disease • Genome wide assoc studies – 16 risk loci • Data supporting Immune-mediation • Presence of autoantibodies (ANCA, ANA, ASMA, and others) • Association with other autoimmune disorders Bacterial/toxin/viral damage and gut microbiota Smoking and coffee appear to be protective
Epidemiology of PSC • Estimated Prevalence in the US: 29,000 (2000) • Estimated Incidence in US: 1 per 100,000 • Males are predominantly affected (2:1) • Occurs in 2-7% of ulcerative colitis patients • 60-80% of PSC cases have ulcerative colitis • Recent study in large cohort of IBD screened with MRCP found a high prevalence (25/322, 7.8%) Bambha K et al. Gastroenterology 2003 Lunder AK, Gastroenterology 2016
Clinical Presentation of PSC • Most patients are asymptomatic at diagnosis • Cholestatic biochemical profile found incidentally in a patient with known IBD • Hypergammaglobulinemia (elevated IgG levels) • Positive ANA, ASMA, pANCA may be found • Symptomatic patients • Most common initial symptoms are abdominal pain (20%), itching (10%), jaundice (6%) and fatigue (6%) • Symptoms of bacterial cholangitis or infection in bile ducts (fever, chills, Abd pain, jaundice)
Mean Liver transplant free survival ~10 years Asymptomatic patients appear to have better survival compared to those with symptoms Natural history of PSC Bambha et al. Gastroenterology 2003
Median Liver transplant free survival was 21.3 years in population based cohort vs. 13.2 yrs in combined LT centers cohort Natural history of PSC Boonstra et al. Hepatology 2013
Diagnosis of PSC • Cholestatic biochemical profile • Characteristic cholangiography (multifocal strictures with segmental dilatations) • Exclusion of secondary causes • Choledocholithiasis, previous biliary surgical trauma, HIV, ischemic stricture post OLT, histiocytosis X, ischemic • Autoantibodies have no role in the diagnosis of PSC
Case scenario • 32 y/o male presents with fatigue, pruritus, abdominal pain, diarrhea. Physical examination unremarkable except for abdominal discomfort. • ALT 43, AST 39, Alk Phosphatase 700, T bili 1.2, INR 1.0, albumin 4.2, AMA negative, ANA negative. Ultrasound shows mild diffuse intrahepatic biliary dilatation, no obvious masses. • What is the next best diagnostic test?
Diagnosis of PSC: Imaging • MRCP: Sensitivity is around 90% and specificity is around 95% • ERCP is the gold-standard for diagnosis • Role of liver biopsy: • Not routinely necessary for the diagnosis of PSC • Often nonspecific, false negatives may occur • Helpful in cholestasis in IBD with normal cholangiogram • Useful in determining stage of fibrosis • Presence of overlap such as autoimmune hepatitis
Special considerations: “Variant forms” IgG-4 associated autoimmune cholangitis Approximately 10% of cases of PSC Increased serum IgG4, bile duct infiltration of IgG4 plasma cells More aggressive course May be steroid-responsive Small duct PSC (5% of patients) Histology typical of PSC with normal cholangiogram Approximately 25% progress to large duct PSC Prognosis is better than classical PSC and cholangiocarcinoma has not been described in small duct PSC PSC with Autoimmune hepatitis features
Autoimmune hepatitis/PSC overlap • Present at a younger age (35% of children with PSC, 5% of adults) and have a worse prognosis when compared to PSC alone • Consider in patients with: • mixed elevation of liver tests + imaging consistent with PSC and serologic suggestive of autoimmune hepatitis (+ANA, + anti-smooth muscle antibody and/or +anti-LKM), elevated IgG levels • Need a liver biopsy for diagnosis • lymphoplasmacytic portal based infiltrates with at least moderate interface hepatitis
Algorithm for the diagnosis of PSC AASLD Guidelines Hepatology 2010;51:660-678
Management of Patients with PSC Role of Endoscopic therapy • Symptoms and Specific • Complications • Pruritus • Fatigue • Bone loss • Fat-soluble vitamin def. • Pre-cirrhotic portal • hypertension possible • Peristomal varices • No proven beneficial • Medical therapy
UDCA in PSC: Effects on Survival Survival Free of Liver Transplantation 105 PSC patients (13-15 mg/kg/d UDCA) Lindor KD, N Engl J Med 1997
High dose UDCA in PSC: 28-30 mg/kg/d Lindor et al. Hepatology 2009
PSC: Future potential therapies • Vancomycin • Vedolizumab (immunosuppressive agent) • All-transretinoic acid (ATRA) • norUDCA • Obeticholic acid • Apical Sodium Dependent Bile Acid Transporter (ASBT) • Antifibrotics (simtuzumab) • Fecal microbiota transplantation
norUDCA improves cholestasis in patients with PSC Fickert et. J Hepatology 2017
PSC: Endoscopic therapy Up to 40% of patients with PSC will develop dominant strictures Stenosis with diameter <1.5mm in the CBD or <1mm in HD Repeated endoscopic interventions are often needed Antibiotic therapy mandatory Stents tend to occlude earlier –exchange in 2 – 3 months Balloon dilatation alone may be preferred Brush cytology and biopsy before endoscopic therapy to exclude malignancy Limitations High grade stenosis >2cm above the bifurcation –consider percutaneous cholangiography
PSC: Liver transplantation Only effective therapy 40% of patients with PSC will ultimately need liver transplantation PSC patients account for 6% of all liver transplants performed in the US Excellent survival rates (85% at 1 year, 72% at 5 years) However, PSC recurs in 15-20% of cases and recurrence may be often associated with loss of the graft
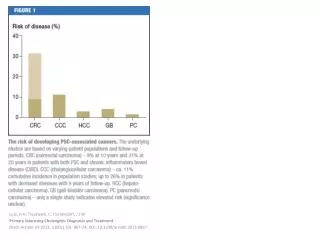
Special considerations Cholangiocarcinoma Annual risk in PSC patients 2% 30-year cumulative risk: approximately 20% 30-50% of patients with cholangiocarcinoma are diagnosed during the following year after PSC diagnosis Guidelines suggested for surveillance based on expert opinion: MRI/MRCP or ultrasound and Ca19-9 annually
Cholangiocarcinoma • High index of suspicion required • Suspect in deteriorating clinical status, worsening liver tests, Ca 19-9 >100 without cholangitis • Imaging –MRI/MRCP • ERCP w/ biopsy and brushings for conventional cytology and fluorescence in situ hybridization (FISH)
PSC-IBD: a unique phenotype • Extensive colitis with rectal sparing – predominantly right sided • Backwash ileitis • Mild or quiescent course • Increased colon cancer risk (RR 4-9) and worsened overall survival vs UC only • Increased risk of pouchitis following IPAA • Increased risk of peristomal varices – avoid ileostomy in PSC patients • Navaneethan U, Shen B Inflamm Bowel Dis 2010
Patient with initial diagnosis of PSC IBD Associated Symptoms Yes No Screening Colonoscopy with Biopsy Diagnosis of IBD No evidence of IBD Screening colonoscopy q 5 years Yearly surveillance colonoscopy for dysplasia IBD-associated symptoms
Surveillance recommendations for patients with PSC Hepatocellular carcinoma Ultrasound every 6 months for cirrhotics Gallbladder cancer Annual US and early cholecystectomy if gallbladder polyps is recommended Colon cancer Patients with PSC & IBD –colonoscopy at diagnosis and every 1-2 yrs Bone health Bone densitometry every 2-3 years
Practical recommendations • Itching – anti-histamines +/- cholestyramine, rifampin --- >check MRCP/ERCP for dominant stricture • New onset jaundice – MRCP/ERCP • Fatigue – Not much to offer • RUQ abdominal pain, fever, jaundice – start ciprofloxacin and call me, consider ERCP • Bone health – calcium supplementation and Vitamin D • Asymptomatic – liver tests every 6 months • Cirrhosis or portal hypertension – surveillance Ultrasound and EGD (varices)
Conclusions • PSC is a rare, chronic, slowly progressive autoimmune liver disease that affects mainly young and middle-aged men, commonly associated with inflammatory bowel disease • No known medical treatment to halt the progression of disease is available; patients may benefit from endoscopic therapy and liver transplantation when appropriate • PSC is associated with a higher life-time risk of hepatobiliary and colorectal malignancies