Download
1 / 33
760 likes | 4.6k Views
Alcoholic liver disease. Alcohol is one of the most common causes of chronic liver diseases. Epidemiology: Alcoholic liver disease occur when patient drink >21U/w in female & 24U/w in male. Most patient with liver disease have drunk heavily > 5 years.

E N D
Alcoholic liver disease • Alcohol is one of the most common causes of chronic liver diseases. Epidemiology: • Alcoholic liver disease occur when patient drink >21U/w in female & 24U/w in male. • Most patient with liver disease have drunk heavily > 5 years. • Average alcohol consumption to develop cirrhosis 160g/d for an average 8ys.
Amount of alcohol in an average drink • Beer:3.5%---------440ml/(1pint) in 2 units 9%-------------9%ml(1pint) in 4 units • Wine:10%-------------10% 125 ml in 1 unit. • Vodka: 37.5%----------25ml in one unit. • Alcopops:6%----------330ml in 2 units
Some of the risk factors for alcoholic liver disease • Drinking pattern. • Gender. • Genetic. • Nutrition.
Aetiology • Alcohol is metabolized almost exclusively by the liver. • 80% of alcohol is metabolized by alcohol dehydrogenase to Acetaldehyde. • Acetaldehyde form adducts with cellular proteins in hepatocytes which activate immune system leading to cell injury. • Acetaldehyde metabolized by Acetaldehyde dehydrogenase to Acetyl Co A & acetate with generation of NADH from NAD.
Pathology • Alcoholic hepatitis: -Lipogranuloma. -Neutrophils infiltration. -Mallory's hyaline. -Pericellular fibrosis. • Macrovesicular steatosis. • Fibrosis & Cirrhosis. • Central hyaline sclerosis.
Clinical features • Asymptomatic. • Abnormal liver function tests. • Cirrhosis. • The liver is often enlarged. • Stigmata of chronic liver disease.
Fatty liver: -Asymptomatic abnormal liver function tests. -Normal /large liver. • Alcoholic hepatitis: -Jaundice. -Malnutrition. -Hepatomegaly. -Features of portal hypertension. • Cirrhosis: -Stigmata of chronic liver disease. -Large , normal or small liver. -ascites , varices, encephalopathy. -Hepatocellular carcinoma.
20% of alcohol is metabolized by Mixed Function Oxidase enzymes in the smooth endoplasmic reticulum Cytochrom CYP2E1. • Microsomal peroxidation lead to oxygen free radicals & mitochondrial damage. • Cytokines:These involved in the fibrogenesis: 1-Increased endotoxines. 2-TNFalpha .from monocytes. 3-Interleukin 1,2 & 8.
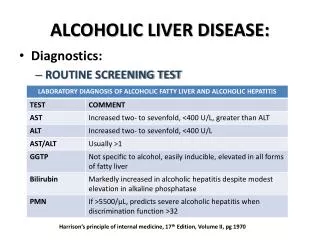
Investigations: Aim: -To establish alcohol misuse. - Exclude alternative or coexistent causes of chronic liver disease. • History of alcohol misuse. • Biochemical markers: Macrocytosis in the absence of anaemia. • Increased GGT is not specific. • Unexplained rib fractures on CXR. • Jaundice suggests alcoholic hepatitis. • Determining the extent of liver damage often required liver biopsy.
Maddreys, score ( discriminant function DF ): enable the clinician to assess prognosis in alcoholic hepatitis. • DF=4.6 x increased in PT (sec.)+ bilirubin (mg/dl) Value >32 = severe liver disease with poor prognosis
Glasgow score: -Age -WBC -Urea -Prothrombin Time -Bilirubin A Score more than 9 is associated with poor prognosis.
Management • Cessation of alcohol consumption is the single most important treatment. • Nutrition: • Corticosteroids: Is of value in severe alcoholic hepatitis. • Pentoxiphylline:has weak anti-TNF action may be beneficial in severe alcoholic hepatitis. • Liver transplantation:
Prognosis • Alcoholic fatty liver disease: Good& steatosis usually disappear after 3 months of abstinence. • Alcoholic hepatitis: Worse prognosis,1/3 die in acute phase. • Alcoholic cirrhosis: 50% only live 5ys.
Non-Alcoholic fatty Liver Disease(NAFLD) The most common cause of chronic liver disease after Hepatitis B & C & alcohol. Classification: Simple fatty liver ( Non-alcoholic fatty liver) Non-alcoholic steatohepatitis (NASH)
Epidemiology: Incidence increased with: • DM& metabolic syndrome. • Drugs: eg.Tamoxifen, Amiodarone. • Exposure to certain Petrochemicals. • Weight reduction , Jejenal bypass surgery.
Aetiology & Pathogenesis • Most patients with NAFLD have insulin resistance. • 2 Hits theory: First hit lead to steatosis ( fatty liver ). If second hit occur ( leptin is needed) to cause hepatic fibrosis.
Clinical features • Asymptomatic with abnormal liver function tests. • Complications of cirrhosis. • Jaundice is only occurred when cirrhosis is established.
Investigations • Liver function tests: • Increased ALT more than AST ( opposite to alcoholic liver disease ) • Increased Alkaline phosphetase in some cases. • Increased transaminases > twice normal + metabolic syndrome ( Hypertriglycerideamia, HT , DM & BMI >25) are useful predictor of NASH.
Ultrasound: Liver looks bright in both NAFL & NASH. • Liver biopsy: Fat deposition is usually macrovesicular . NASH is characterized by neutrophils infiltration & pericellular fibrosis like alcohol liver disease but diagnosis of NASH depend on: - Absence of alcohol drinking. - Absence of jaundice. - Presence of risk factors like obesity ,DM.
Management • Decreased BMI & Insulin resistance. • Metformine: Improve LFTs & is first choice for DM & NAFLD. • Thiazolidinediones : as ( Proglitazone ) improve LFTs in NAFLD & may improve inflammation & fibrosis. • Antioxidants: As Vitamin E are not effective. • No rational to use HMG Co A reductase Inhibitors statine in the treatment of NAFLD, but for coexistent hyperlipidaemia.
Prognosis • Once cirrhosis occurred survival is similar to hepatitis induced cirrhosis. • Hepatocellular carcinoma complicate NAFLD induce cirrhosis.
Drugs ,Toxins & the liver • The liver is the primary site of drug metabolism. • Liver disease may affect the capacity of the liver to metabolize drugs . • Unexpected toxicity may occur when patients with chronic liver disease are given drugs in normal doses.
Hepatotoxic drug reaction • Example of common causes of drug-induced hepatotoxicity: -- Cholestatic:----------------- ---------------Chlorpromazine. High dose estrogens. -- Cholestatic hepatitis: ------------------ NSAIDs Co-Amoxiclav Statins -- Acute hepatitis:------------------------- Rifampicin INH -- Non-alcoholic steatohepatitis: -----Amiodarone -- Venous outflow obstruction:--------Busulfan Azathioprine -- Fibrosis:------------------------------------Methotrexate
Most drug reactions are acute & self limiting & chronic liver damage is rare. • LFTs take weeks to return to normal drug induced hepatitis & it may take months following cholestatic hepatitis.
The diagnosis of acute drug induced liver disease • Tabulate drug taken: prescribed ,self administered. • Establish if reported hepatotoxicity in the literature. • Relate time taken to onset of illness (4ds-8ws) usual. • Effect of stopping drugs on normalization of liver biochemistry. Hepatitis LFTs(2Ms),Cholestatic/Mixed LFTs(6Ms). • Exclude other causes: like viral hepatitis, biliary disease. • Consider liver biopsy. N.B: Challenge tests with drugs should be avoided.
Types of liver injury • Cholestasis: -- Estrogen in higher concentration. -- Chlorpromazine, Flucloxacillin cause cholestatic hepatitis. -- Amoxiclav is the most common antibiotic that cause abnormal LFTs ,but it may not produce symptoms until 10-42 days after it is stopped. -- Anabolic steroid cause cholestatic hepatitis.
Hepatocytes necrosis: with high serum transaminase concentration -- Paracetamol. -- NSAIDs. -- INH. -- Allopurinol : Cause granuloma. -- Herbal remedies. -- Cocaine.
Steatosis: -- Microvesicular steatosis due to effect on mitochondrial beta-oxidation. -- Tetracycline. -- Na Valproate. -- Tamoxifen. -- Amiodarone.
Vascular / Sinusoidal lesions: -- Alkylating agents: cause hepatic venous outflow obstruction. -- Chronic over dose of Vitamin A: Cause portal hypertension. • Hepatic fibrosis: -- Methotrexate :cause cirrhosis when used in high dose over a long time. Risk factors include: preexisting liver disease & high alcohol intake.
Drugs should be a voided in cirrhosis • NSAIDs: Decrease renal bl. Flow & Hepatorenal failure. Ulceration cause bleeding varices. • ACE Inhibitors: decrease renal bl.flow: Hepatorenal failure. • Codeine: Constipation: Hepatic encephalopathy. • Narcotics: Constipation & drug accumulation: Hepatic encephalopathy • Anxiolytics: Drug accumulation & hepatic encephalopathy