Download

1 / 38
470 likes | 1.93k Views
Buffy Coat Component Production . 2009 Medical Residents. Outline. Background on buffy coat production method Description of the buffy coat production method Clinical implications. Background.

E N D
Buffy Coat Component Production 2009 Medical Residents
Outline • Background on buffy coat production method • Description of the buffy coat production method • Clinical implications
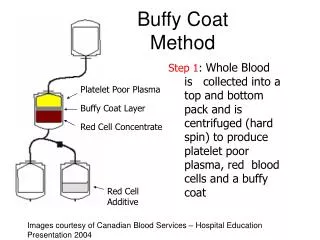
Background • “Buffy Coat” refers to a method for preparing components from whole blood donation that was developed in Europe >25 years ago and is in widespread use around the world. • In this method whole blood is spun down hard and three distinct layers can be seen. The middle “buff” coloured layer is made of White Cells and Platelets and rests on top of the RBC layer or “coats” the RBC layer
Potential Future Benefits • Platelets prepared by BC method can be suspended in platelet additive solutions. These solutions improve platelet quality to the level required to extend platelet storage beyond 7 days. This will be investigated by CBS R&D group at a later date. • Pathogen reduction/inactivation technologies for platelets have been designed only for apheresis or buffy coat platelet products.
Key Benefits – cooling trays • Increase in time allowed for component production (24 hours vs. 8 hours) through the use of a rapid cooling technique • improves availability of platelets
Key Benefits – automated extraction • Instrument-controlled extraction allows for increased process control better quality product more consistent recoveries therefore more consistent platelet dose higher percentage of platelets recovered per donation
Key Benefits – sterile docking • Hospitals receive a pooled platelet concentrate that has been produced in a closed system. • Less donor exposure for recipients – 4 donations pooled instead of 5 • Product is pooled in plasma from male donors to reduce the risk of TRALI
Benefits for CBS = Benefits for Hospitals • Increased volume of Recovered Plasma • approx. 70-80 mL/donation • reduces Canada’s dependency on open market IVIG, improving security of supply and reducing overall cost to the health care system
Medical Overview Yes • Key Questions • Will the Buffy Coat Product work as well as the previous product? • Will there be an increase in adverse reactions? • Are there different anti-coagulants and will they effect neonatal practice? • Will there be changes to Autologous and Directed Components? • Do I need to change my blood prescription practice? • Do we need to test pooled buffy coat platelets for hemolysins? • After buffy coat implementation will all platelets produced by CBS be routinely bacterially tested? • Are there any differences on the ward? No Yes and No Yes - Packed Red Blood Cells now Maybe for platelets and plasma Maybe – if this is part of your apheresis platelet routine Yes No, provided “correct” spiking method is used
Hb content of RBC units *QC results from Edmonton (6 months 2008)
Anticoagulant in Whole blood Derived Plasma* * Data provided by bag manufacturer
RBC Preservative Solution* (continued) *Vox Sang 1998; 74 (Suppl 2) : 177-187, Preparation and Preservation of Red Cells, C.F. Hogman
Frozen plasma from whole blood donations change from 8 to 24 hours hours
FFP current method 8 hours after collection FP produced from BC 20-24 hrs after collection Mean Std Dev Mean Std Dev NL Range Factor X 1.24 0.164 1.07 0.164 0.50 - 1.50 U Factor XI 1.11 0.161 0.94 0.151 0.50 - 1.50 U Factor II 1.12 0.137 0.95 0.123 0.50 - 1.50 U Factor V 1.15 0.189 1.06 0.192 0.50 - 1.50 U Factor VII 1.09 0.230 0.90 0.207 0.50 - 1.50 U Factor VIII 1.26 0.315 0.91 0.250 0.50 - 1.50 U Factor IX 1.03 0.142 0.87 0.188 0.50 - 1.50 U FFP vs BC FP Protein Function (ABO matched, n=20) Note: small data sample size may not be reflective of current performance.
Produced from PRP within 10 hours of collection Produced from BC 20-24 hrs after collection Mean Std Dev Mean Std Dev NL Range Antithrombin 0.97 0.078 1.01 0.053 >0.75 U Protein C 1.19 0.223 1.05 0.122 >0.70 U Fibrinogen 3.01 0.481 3.92 1.945 2.00 - 5.00 g/L Protein S 1.15 0.472 1.03 0.180 >0.65 U Von Willebrand 1.24 0.405 1.13 0.377 >0.50 U Alpha 2 Antiplasmin 1.01 0.084 0.96 0.084 --------- FFP vs BC FP Protein Function (ABO matched, n=20) Note: small data sample size may not be reflective of current performance.
Results* **No high molecular weight bands seen in any CSP plasma product *Results are reported as mean with result in brackets to show range
Platelet counts in buffy coat platelet pools (pools of 4) *QC results from Edmonton (last 6 months) • Council of Europe standard • - BC: > 6.0 x 1010/single unit equivalent; 1% of units • CSA standard • - PRP: > 5.5 x 1010/unit in 75% of units tested • (4 or 5 x 5.5 x 1010 = 2.2 or 2.75 x 1011) • - Apheresis units: 3 x 1011/unit in 75% of units tested
Platelet dose for neonates & infants • Neonatal platelet dose • 10-20 ml per kg • Preterm infants can weigh less than 1 kg • Pediatric platelet dose • 5-10 ml per kg, or • 1 unit per 10 kg
Platelets for neonates & infants • Three types of platelet concentrates will be available: 1. Single units of PRP platelets 2. An aliquot of an apheresis unit that has been prepared sterilely to allow for: • Storage of the remainder of the apheresis unit • pH must be > 6.2 (6.8 – 7.4) • max platelet concentration 1.5 x 109/ml • information from manufacturer for apheresis units – conditions are met if remaining volume > 100 ml 3. An aliquot from a BC unit • vendor storage requirements for remainder of bag contents
Hospital Impacts - Spiking • Lack of awareness of different technique to access ports and spike. Some hospitals had difficulty spiking and required vendor training sessions during Edmonton pilot (October 2005). • Changes since Edmonton pilot • Port diameter increased to reduce spiking difficulties • Where difficulties identified with specific transfusion sets, vendors will provide alternate products • Implementation of ISO standard Pall medical bags has occurred which require the different technique • Hospitals were notified to assess needs at least 5 months prior to implementation
Trouble Shooting Tips for Spiking 1. Do not over spike. Over-spiking will result in the inability to remove the set. 2. Always insert/remove spike using ¼ turn motions. Pulling the spike in a straight downward motion will result in the tightening of the port on the spike.
Medical Overview Yes • Key Questions • Will the Buffy Coat Product work as well as the previous product? • Will there be an increase in adverse reactions? • Are there different anti-coagulants and will they effect neonatal practice? • Will there be changes to Autologous and Directed Components? • Do I need to change my blood prescription practice? • Do we need to test pooled buffy coat platelets for hemolysins? • After buffy coat implementation will all platelets produced by CBS be routinely bacterially tested? • Are there any differences on the ward? No Yes and No Yes packed cells now Maybe for platelets and plasma Maybe – if this is part of your apheresis platelet routine Yes No, provided “correct” spiking method is used
Additional resources • CBS Circular of Information • www.transfusionmedicine.ca • www.blood.ca