Download
1 / 26
260 likes | 378 Views
Computerized Chemotherapy Order Entry (COE) Lessons Learned from Development, Implementation and Maintenance. Lawrence N Shulman, MD Dana-Farber Cancer Institute Brigham and Women’s Hospital. Critical Components for Developing COE. High level support Administrative leadership

E N D
Computerized Chemotherapy Order Entry (COE)Lessons Learned from Development, Implementation and Maintenance Lawrence N Shulman, MD Dana-Farber Cancer Institute Brigham and Women’s Hospital
Critical Components for Developing COE High level support • Administrative leadership • Clinical leadership • Financial support • Programmatic support • Atmosphere of “this will happen” – life is not a democracy • Fair and Just Culture
Basic Principles for Chemotherapy Ordering and Administration Shared responsibility • Physicians, nurses, and pharmacists all assume “complete” responsibility • No group abdicates responsibility for any component of care • Atmosphere where communication, questioning, and discussion are supported • Ultimately, senior clinicians, administrators and trustees accept responsibility for actions of staff
COE Implementation and Continued Development – The Team Multidisciplinary team • Co-leaders – MD/IS analyst/IS programmer • MDs – clinicians, representatives from P&T, and fellows • Nursing • Pharmacy leadership and staff • IS staff – analysts, programmers and “builders” • Protocol office Frequent meetings – 2x/month x 10 yrs, now once/month Equal voice for all at table
COE- Principles of Implementation and Continued Development • Compartmentalized risk analysis and approach • Automation of any component of work possible • Iterative process
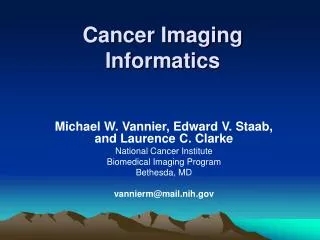
Process #1 Error Rate 1/10 Process #2 Error Rate 1/10 Process #3 Error Rate 1/10 Overall Error Rate 3/10 (30%)
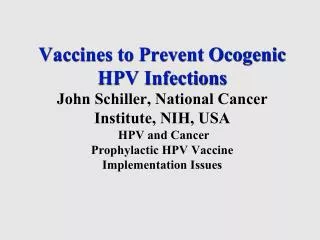
3 People involved Error Rate 1/10 for each Overall Error Rate 1/1000 Process #1 Process #2 Process automated Error rate 0 3 People involved Error Rate 1/10 for each Overall Error Rate 1/1000 Process #3 Overall Error Rate 2/1000 (0.2%)
COE – Iterative Process of Development and Deployment • Don’t attempt to develop ‘ideal’ system before deployment • What are the minimal requirements to implement the next system/step? • Look for incremental improvements in safety • Priority lists – and continuous re-evaluation, related to Interventions program and “error events” • Continuous development – for ever!!
COE- Principles of Implementation and Continued Development Safety over convenience • Conscious decision issue by issue Reduction in ambiguity • Hydration and criteria to initiate treatment Standardization Conscious evaluation of work flow effects • Looking for trade-offs – what can a system do to aid clinicians as well as enhance safety?
COE- Principles of Implementation and Continued Development Standardization!! Templated Treatment Regimens • Consensus on accepted regimens for each disease group • Consensus on specifics of each regimen (one CMF) • Recommended antiemetics included • All necessary ancillary meds included • Recommended hydration orders included
COE- Principles of Implementation and Continued Development Patients linked to approved investigational protocol registration • Pts registered through protocol office who reviews consent and eligibility criteria • Protocol office assigns pt to protocol and specifics of treatment auto-templated into orders including assignment to specific treatment “arm”
Patient Safety – IT Infrastructure Availability of All Necessary Patient Data • Integrated systems • Clinician documentation – MD/RN/etc – electronic medical record • Lab, radiology, pathology data • On-line ordering treatment regimens • On-line protocols and consents – NO paper copies as primary source • On-line consent verification • Universal protocol-enrollment notification in electronic record, chemotherapy order entry system, etc
Jane Doe Jane Doe
Jane Doe Jane Doe
COEContinuous Quality Improvement Fair and Just Culture (non-punitive) • Support for error identification • Definition of errors – concentrating on potential errors – “near misses” – those that are caught and do not reach the pt • Concentration on systems – not individuals • Root Cause Analysis system for serious errors • Need to sort out truly problematic individuals
COE – Response to Major Errors The RCA Process • SWAT team – meets on short notice • Convener and Facilitator • High level clinical and administrative participation • Multidisciplinary • Ideally, those who need to be present to make decisions are involved • Focuses on systems, not individuals • Reports to MSEC • Reports to Board level QI/Risk Management Committee
COE – Continuous Cycle Improvement The Interventions Program • Facile reporting mechanism for staff • Nursing, pharmacy, etc • Non-punitive – staff have told us this will stop if they fear punitive action for their colleagues • Tabulation and analysis of data to look for trends – by P&T committee and results, without clinician identification, given to COE team • Rounding system – “What has occurred today that worries you about pt safety?” • Reports to MSEC • Reports to Board level QI/Risk Management Committee
Patient SafetyPatient Involvement makes it better • Patients involved at all levels, including in meetings with leadership and trustees • Identification of risk issues (they see things we sometimes miss – and often have business background with experience in systems) • Identification of potential solutions • Medication error project • High level committees including trustee level QI Risk Management committee • By-in of patients when changes are made • Patients not involved in RCA (peer review issues)
Patient Safety Full disclosure of errors to patients and families • Institute policy • Must be timely • Must be complete • Institute support for those involved • Positive outcomes
Computerized Chemotherapy Order Entry System as a Model • All in all - a success • Involvement of all needed parties • Culture of safety, risk-mitigation, and cooperation of all groups • Culture of continuous improvement – there is always something that can be done better • It has been both fun and rewarding