Download
1 / 20
200 likes | 333 Views
HIV Cases “What to Start”. Dr Anton Pozniak Chelsea and Westminster Hospital London. Case-SP. A 57 year old caucasian man presented to the emergency department with progressive difficulty in swallowing over the last 4 weeks.

E N D
HIV Cases“What to Start” Dr Anton Pozniak Chelsea and Westminster Hospital London
Case-SP • A 57 year old caucasian man presented to the emergency department with progressive difficulty in swallowing over the last 4 weeks. • He is hypertensive and has diet controlled diabetes and asthma and takes inhaled B2 agonists and inhaled steroids • He had seen his family practitioner who saw oral thrush and thought it was related to his diabetes/ inhalers and gave him amphotericin lozenges • He had been diagnosed with HIV a year before but had not attended any clinics as he “felt well”
Case-SP • He had extensive oral thrush and had severe dysphagia • BP 145/90 mmHg • He was admitted and treated with fluconazole • Social History • Lives alone is MSM • Smokes 15 a day • Alcohol 20 units a week, no recreational drugs • Drugs • Salbutamol inhaler • Fluticasone Inhaler • Amlodopine • St Johns Wort for depression
Case-SP • Labs • STD screen negative • FBC,U and Es, LFTs Normal , • Cr CL 69 mls/min, Urine protein +no glucose • CD4 33 cells/uL • VL 365000 copies/ml • Hep B immune • Hep C negative • STS negative • Resistance test and HLA B5701 awaited • Framingham 10 year risk risk 18%
You decide to start ARVs 1. DHHS Guidelines, March 2012. 2. T. JAMA. 2012;304:321-333. 3. EACS Guidelines, November 2011.
You decide to start ARVs What is your choice of main agent? • NNRTI • PI/r • Integrase • other
Difficulties in choosing-which 3rd agent? • NNRTI- • may have transmitted dug resistance • RPV may not be effective in High viral load • Integrase • BD • and may have NRTI transmitted dug resistance • PI/r • drug interactions, • diabetes, lipids
NNRTI/NRTI and Prevalence of Transmitted Drug Resistance Eacs 2011 SPREAD
If you decide to give a boosted PIDrug Interactions • What Drugs have significant interactions with a boosted PI? 1 St Johns Wort 2 Fluticasone 3 Amlodopine 4 None 5 all
What NRTI back bone? • AZT/3TC • ABC/3TC • TDF/FTC • DDI/3TC • OTHER
Difficulties in choice of NRTI • AZT- • lipodystrophy • BD • ABC • High Viral load • Cardiovascular risk(smoker and diabetic and BP) • TDF • Renal changes, • Bone changes
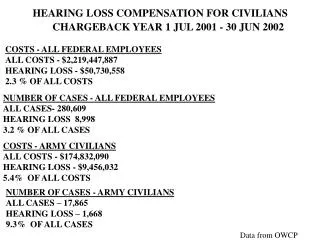
CVD – Do drugs matter? D:A:D: Recent and/or cumulative ARV exposure and risk of MI RR of cumulative exposure/year95%CI NRTI 1.9 1.9 RR of recent* exposureyes/no95%CI 1.5 1.5 1.2 1.2 ** 1.0 1.0 0.8 0.8 0.6 0.6 ZDV ddI ddC d4T 3TC ABC TDF # PYFU: 138,109 74,407 29,676 95,320 152,009 53,300 39,157# MI: 523 331 148 405 554 221 139 RR of cumulative exposure/year95%CI NNRTI PI† 1.2 1.13 1.1 1.0 0.9 IDV NFV LPV/RTV SQV NVP EFV # PYFU: 68,469 56,529 37,136 44,657 61,855 58,946# MI: 298 197 150 221 228 221 *Current or within past 6 months; †Approximate test for heterogeneity: p=0.02; **not shown due to low number of patients receiving ddC CVD=cardiovascular disease; ARV=antiretroviral; MI=myocardial infarction; RR=relative risk; NRTI=nucleoside reverse transcriptase inhibitor; PI=protease inhibitor; NNRTI=nonnucleoside reverse transcriptase inhibitor; PYFU=patient years of follow up Adapted from Lundgren JD, et al. CROI 2009. Oral presentation 44LB.
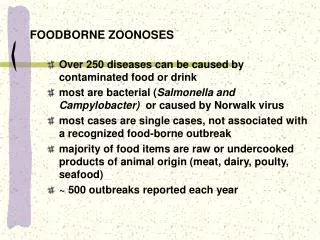
CVD: Do drugs matter? FDA meta-analysis of abacavir and MI Mantel-Haenszel Risk Difference % (95% CI) • Meta-analysis of Phase II–IV RCTs including ABC • Mean follow up 1.6 person-years per subject • Patients: 80% male (mean age=39 years) • Limitations • Young adults, so underlying MI risk low • Other CV risk factors usually unknown • Unvalidated MIs • Some studies had a PI control group Academic Trials n=5 -0.53 0.31 1.16 NIH Trials n=5 -0.45 0.03 0.51 GSK Trials n=16 -0.43 -0.11 0.21 All Trials n=26 0.008 -0.26 0.27 CVD=cardiovascular disease; FDA=Food and Drug Administration; MI=myocardial infarction; RCTs=randomised controlled trials; CV=cardiovascular; PI=protease inhibitor -0.8 0.4 0.8 1.2 -0.4 0 Created from Ding X, et al. CROI 2011. Poster presentation 808.
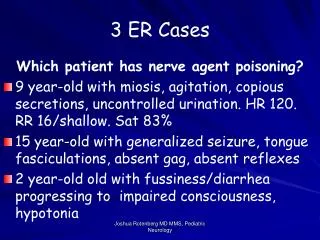
Chronic renal disease: ART risk factors • 6,843 patients (5,136 male), median age 43 yrs, 90.1% exposed to cART, CD4 450 cells/mm3, 21.7% hypertension, 4.9% diabetes • Median follow up 3.7 years • 2-fold increased risk if hepatitis C RNA+ Incidence: 1.05 (0.91–1.18)/100 PYFU % progressed to CKD Months ART=antiretroviral therapy; PYFU=patient years follow up; IRR=incidence rate ratio Adapted from Mocroft A, et al. AIDS. 2010;24:1667–8.
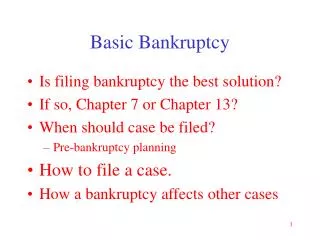
Low bone density/fracture: Relationship to ART ACTG 5224 & SMART: BMD loss with ART initiation ~2-4% at 1-2 yrs1 NRTI Component Primary Analysis NNRTI/PI Component Secondary Analysis EFV TDF/FTC ATV/rtv ABC/3TC 0 0 p=.004* p=.004* p=.035* -1 -1 Spine BMD percent change from week 0 -2 -2 -3 -3 -4 -4 -5 -5 24 96 144 192 0 48 0 48 24 96 144 192 Visit Week from Randomization Visit Week from Randomization No. of subjects No. of subjects TDF/FTC 128 111 105 97 87 53 EFV 133 117 109 107 86 58 ABC/3TC 122 53 ATV/rtv 116 48 130 106 101 80 125 102 91 81 * - two-sample t-test No significant interaction of NRTI and NNRTI/PI components (p=0.63) ART=antiretroviral therapy; BMD=bone mineral density; DC=drug conservation; VS=viral suppression; NRTI=nucleoside reverse transcriptase inhibitor; NNRTI=nonnucleoside reverse transcriptase inhibitor; PI=protease inhibitor; DXA=dual-energy X-ray absorptiometry 1. Adapted from McComsey G, et al. JID. 2011;203:1791–801.
Case-SP • Resistance was wild type • He starts EFV TDF FTC
Case AP • 35 year old Asian women presents with • Night sweats, weight loss and cough • CXR - RUL cavity and infiltrates • AAFB - smear positive and started on RZHE • Had an HIV test and was positive CD4 was 35 cells/uL
Case AP • As her CD4 was<50 cells/uL she was offered ARVs within 2 weeks of starting and tolerating her TB meds What ARV combination would you offer her? What is your choice of main agent? • NNRTI-Efavirenz • PI/r-Lopinavir/r • Integrase-Raltegravir • other
Case AP • Started Efavirenz but couldn't tolerate it • What would you offer her? • NNRTI-Nevirapine • PI/r-Lopinavir/r • Integrase-Raltegravir • other
Case AP • What would you offer her? • NNRTI-Nevirapine-less efficacy ? Drug interaction • PI/r-Lopinavir/r major interaction with rifampicin so switch to rifabutin or double dose lopinavir/r or high dose ritonavir 400mg bd • Integrase-Raltegravir 400 or 800mg bd • Other-4 nucleosides