Download
1 / 1
10 likes | 206 Views
After Controlling for Poor Effort, Veterans with PTSD and/or a History of mTBI Show No Evidence of Cognitive Impairment John Denning, Ph.D. TN Valley Healthcare System, Alvin C. York VA Hospital, Murfreesboro, TN. Poor Effort PTSD mTBI Both

E N D
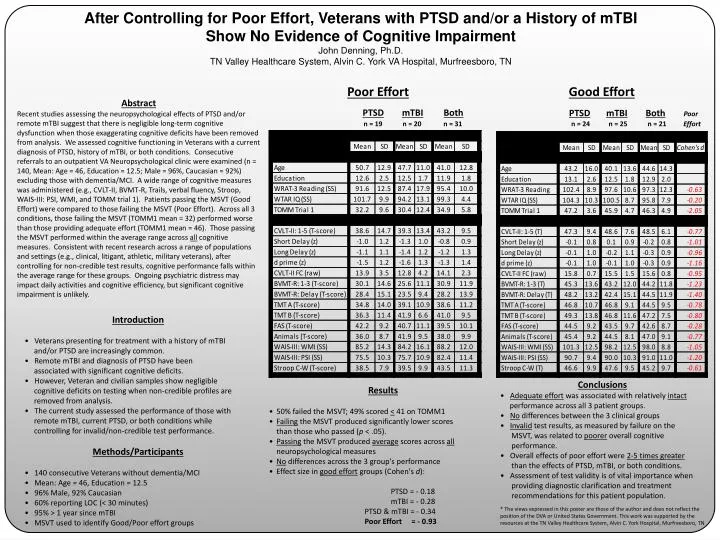
After Controlling for Poor Effort, Veterans with PTSD and/or a History of mTBI Show No Evidence of Cognitive Impairment John Denning, Ph.D. TN Valley Healthcare System, Alvin C. York VA Hospital, Murfreesboro, TN Poor Effort PTSDmTBIBoth n = 19 n = 20 n = 31 Good Effort PTSDmTBIBothPoor n = 24 n = 25 n = 21 Effort Abstract Recent studies assessing the neuropsychological effects of PTSD and/or remote mTBI suggest that there is negligible long-term cognitive dysfunction when those exaggerating cognitive deficits have been removed from analysis. We assessed cognitive functioning in Veterans with a current diagnosis of PTSD, history of mTBI, or both conditions. Consecutive referrals to an outpatient VA Neuropsychological clinic were examined (n = 140, Mean: Age = 46, Education = 12.5; Male = 96%, Caucasian = 92%) excluding those with dementia/MCI. A wide range of cognitive measures was administered (e.g., CVLT-II, BVMT-R, Trails, verbal fluency, Stroop, WAIS-III: PSI, WMI, and TOMM trial 1). Patients passing the MSVT (Good Effort) were compared to those failing the MSVT (Poor Effort). Across all 3 conditions, those failing the MSVT (TOMM1 mean = 32) performed worse than those providing adequate effort (TOMM1 mean = 46). Those passing the MSVT performed within the average range across all cognitive measures. Consistent with recent research across a range of populations and settings (e.g., clinical, litigant, athletic, military veterans), after controlling for non-credible test results, cognitive performance falls within the average range for these groups. Ongoing psychiatric distress may impact daily activities and cognitive efficiency, but significant cognitive impairment is unlikely. • Introduction • Veterans presenting for treatment with a history of mTBI • and/or PTSD are increasingly common. • Remote mTBI and diagnosis of PTSD have been • associated with significant cognitive deficits. • However, Veteran and civilian samples show negligible • cognitive deficits on testing when non-credible profiles are • removed from analysis. • The current study assessed the performance of those with • remote mTBI, current PTSD, or both conditions while • controlling for invalid/non-credible test performance. • Methods/Participants • 140 consecutive Veterans without dementia/MCI • Mean: Age = 46, Education = 12.5 • 96% Male, 92% Caucasian • 60% reporting LOC (< 30 minutes) • 95% > 1 year since mTBI • MSVT used to identify Good/Poor effort groups • Conclusions • Adequate effort was associated with relatively intact • performance across all 3 patient groups. • No differences between the 3 clinical groups • Invalid test results, as measured by failure on the • MSVT, was related to poorer overall cognitive • performance. • Overall effects of poor effort were 2-5 times greater • than the effects of PTSD, mTBI, or both conditions. • Assessment of test validity is of vital importance when • providing diagnostic clarification and treatment • recommendations for this patient population. • * The views expressed in this poster are those of the author and does not reflect the position of the DVA or United States Government. This work was supported by the resources at the TN Valley Healthcare System, Alvin C. York Hospital, Murfreesboro, TN • Results • 50% failed the MSVT; 49% scored < 41 on TOMM1 • Failing the MSVT produced significantly lower scores • than those who passed (p < .05). • Passing the MSVT produced average scores across all • neuropsychological measures • No differences across the 3 group's performance • Effect size in good effort groups (Cohen's d): • PTSD = - 0.18 • mTBI = - 0.28 • PTSD & mTBI = - 0.34 • Poor Effort = - 0.93



















