Download
1 / 1
10 likes | 130 Views
Collaborative Care: Depression Initiative in Primary care (CC: DIP) Van der Feltz-Cornelis CM, Van Marwijk HWJ, Huijbregts KML, IJff MA, Nijpels G, Beekman AJ. Screening Procedure: Fase1: Screening with PHQ-9 using the GP’s database. Fase2: Classification with MINI-

E N D
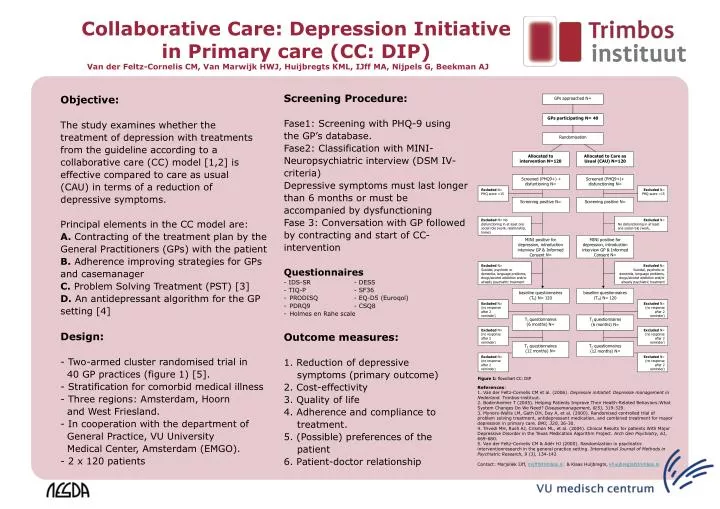
Collaborative Care: Depression Initiative in Primary care (CC: DIP) Van der Feltz-Cornelis CM, Van Marwijk HWJ, Huijbregts KML, IJff MA, Nijpels G, Beekman AJ • Screening Procedure: • Fase1: Screening with PHQ-9 using • the GP’s database. • Fase2: Classification with MINI- • Neuropsychiatric interview (DSM IV- • criteria) • Depressive symptoms must last longer • than 6 months or must be • accompanied by dysfunctioning • Fase 3: Conversation with GP followed • by contracting and start of CC- • intervention • Questionnaires • - IDS-SR - DESS • - TIQ-P - SF36 • PRODISQ - EQ-D5 (Euroqol) • PDRQ9 - CSQ8 • Holmes en Rahe scale • Outcome measures: • Reduction of depressive • symptoms (primary outcome) • 2. Cost-effectivity • 3. Quality of life • 4. Adherence and compliance to • treatment. • 5. (Possible) preferences of the • patient • 6. Patient-doctor relationship Objective: The study examines whether the treatment of depression with treatments from the guideline according to a collaborative care (CC) model [1,2]is effective compared to care as usual (CAU) in terms of a reduction of depressive symptoms. Principal elements in the CC model are: A. Contracting of the treatment plan by the General Practitioners (GPs) with the patient B. Adherence improving strategies for GPs and casemanager C. Problem Solving Treatment (PST) [3] D. An antidepressant algorithm for the GP setting [4] Design: - Two-armed cluster randomised trial in 40 GP practices (figure 1) [5]. - Stratification for comorbid medical illness - Three regions: Amsterdam, Hoorn and West Friesland. - In cooperation with the department of General Practice, VU University Medical Center, Amsterdam (EMGO). - 2 x 120 patients References: 1. Van der Feltz-Cornelis CM et al. (2006). Depressie initiatief. Depressie management in Nederland. Trimbos-instituut. 2. Bodenheimer T (2005). Helping Patients Improve Their Health-Related Behaviors:What System Changes Do We Need? Diseasemanagement, 8(5), 319-329. 3. Mynors-Wallis LM, Gath DH, Day A, et al. (2000). Randomised controlled trial of problem solving treatment, antidepressant medication, and combined treatment for mayor depression in primary care. BMJ, 320, 26-30. 4. Trivedi MH, Rush AJ, Crismon ML, et al. (2004). Clinical Results for patients With Major Depressive Disorder in the Texas Medication Algorithm Project. Arch Gen Psychiatry, 61, 669-680. 5. Van der Feltz-Cornelis CM & Adèr HJ (2000). Randomization in psychiatric interventionresearch in the general practice setting. International Journal of Methods in PsychiatricResearch, 9 (3), 134-142 Contact: Marjoliek IJff, mijff@trimbos.nl & Klaas Huijbregts, khuijbregts@trimbos.nl