Download
1 / 1
10 likes | 151 Views
A Novel Approach to Teaching Communication: Using the Cognitive-Behavioural Model (CBM) Claire De Souza 1 , Melinda Solomon 2 1. Pediatric Psychiatrist; 2. Pediatric Respirologist Hospital for Sick Children, University of Toronto, Toronto, Canada. Background. Objectives. Questionnaire.

E N D
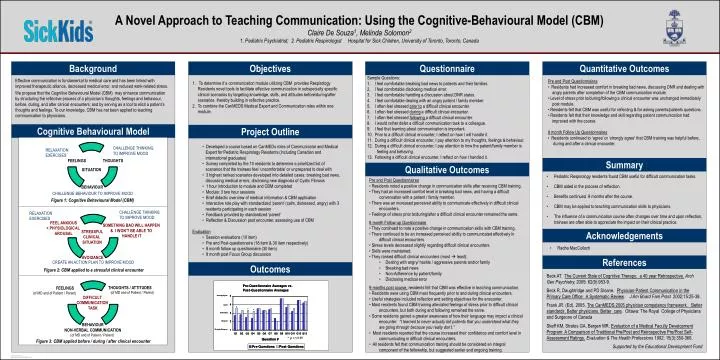
A Novel Approach to Teaching Communication: Using the Cognitive-Behavioural Model (CBM) Claire De Souza1, Melinda Solomon2 1. Pediatric Psychiatrist; 2. Pediatric Respirologist Hospital for Sick Children, University of Toronto, Toronto, Canada Background Objectives Questionnaire Quantitative Outcomes • Sample Questions: • I feel comfortable breaking bad news to patients and their families. • I feel comfortable disclosing medical error. • I feel comfortable handling a discussion about DNR status. • I feel comfortable dealing with an angry patient / family member. • I often feel stressed prior to a difficult clinical encounter. • I often feel stressed during a difficult clinical encounter. • I often feel stressed following a difficult clinical encounter. • I would rather defer a difficult communication task to a colleague. • I feel that learning about communication is important. • Prior to a difficult clinical encounter, I reflect on how I will handle it. • During a difficult clinical encounter, I pay attention to my thoughts, feelings & behaviour. • During a difficult clinical encounter, I pay attention to how the patient/family member is • feeling and behaving. • 13. Following a difficult clinical encounter, I reflect on how I handled it. Effective communication is fundamental to medical care and has been linked with improved therapeutic alliance, decreased medical error, and reduced work-related stress. We propose that the Cognitive Behavioural Model (CBM) may enhance communication by structuring the reflective process of a physician’s thoughts, feelings and behaviour, before, during, and after clinical encounters; and by serving as a tool to elicit a patient’s thoughts and feelings. To our knowledge, CBM has not been applied to teaching communication to physicians. 1. To determine if a communication module utilizing CBM provides Respirology Residents novel tools to facilitate effective communication in subspecialty specific clinical scenarios by targeting knowledge, skills, and attitudes before/during/after scenarios, thereby building in reflective practice. 2. To combine the CanMEDS Medical Expert and Communication roles within one module. • Pre and Post Questionnaires • Residents had increased comfort in breaking bad news, discussing DNR and dealing with • angry parents after completion of the CBM communication module. • Level of stress prior to/during/following a clinical encounter was unchanged immediately • post module. • Residents felt that CBM was useful for reflecting & for asking parents/patients questions. • Residents felt that their knowledge and skill regarding patient communication had • improved with the course. • 8 month Follow Up Questionnaires • Residents continued to ‘agree’ or ‘strongly agree’ that CBM training was helpful before, • during and after a clinical encounter. Cognitive Behavioural Model Project Outline • Developed a course based on CanMEDs roles of Communicator and Medical • Expert for Pediatric Respirology Residents (including Canadian and • international graduates) • Survey completed by the 10 residents to determine a prioritized list of • scenarios that the trainees feel ‘uncomfortable’ or unprepared to deal with • 3 highest ranked scenarios developed into detailed cases: breaking bad news, • discussing medical errors, disclosing new diagnosis of Cystic Fibrosis • 1 hour introduction to module and CBM completed • Module: 3 two hour sessions • Brief didactic overview of medical information & CBM application • Interactive role play with standardized ‘parent’ (calm, distressed, angry) with 3 • residents participating in each session • Feedback provided by standardized ‘parent’ • Reflection & Discussion post encounter, assessing use of CBM • Evaluation • Session evaluations (10 item) • Pre and Post-questionnaire (18 item & 30 item respectively) • 8 month follow up questionnaire (30 item) • 9 month post Focus Group discussion CHALLENGE THINKING TO IMPROVE MOOD RELAXATION EXERCISES FEELINGS THOUGHTS Summary Qualitative Outcomes SITUATION • Pediatric Respirology residents found CBM useful for difficult communication tasks. • CBM aided in the process of reflection. • Benefits continued 9 months after the course. • CBM may be applied to teaching communication skills to physicians. • The influence of a communication course often changes over time and upon reflection, trainees are often able to appreciate the impact on their clinical practice. • Pre and Post Questionnaires • Residents noted a positive change in communication skills after receiving CBM training. • They had an increased comfort level in breaking bad news, and having a difficult • conversation with a patient / family member. • There was an increased perceived ability to communicate effectively in difficult clinical • encounters. • Feelings of stress prior to/during/after a difficult clinical encounter remained the same. • 8 month Follow-up Questionnaire • They continued to note a positive change in communication skills with CBM training. • There continued to be an increased perceived ability to communicated effectively in • difficult clinical encounters. • Stress levels decreased slightly regarding difficult clinical encounters. • Skills were maintained. • They ranked difficult clinical encounters (most least): • Dealing with angry/ hostile / aggressive parents and/or family • Breaking bad news • Non-Adherence by patient/family • Disclosing medical error • 9 months post course, residents felt that CBM was effective in teaching communication. • Residents were using CBM most frequently prior to and during clinical encounters. • Useful strategies included reflection and setting objectives for the encounter. • Most residents found CBM training alleviated feelings of stress prior to difficult clinical • encounters, but both during and following remained the same. • Some residents gained a greater awareness of how their language may impact a clinical • encounter: “I learned to never actually tell patients that you understand what they • are going through because you really don’t.” • Most residents reported that the course increased their confidence and comfort level in • communicating in difficult clinical encounters. • All residents felt that communication training should be considered an integral • component of the fellowship, but suggested earlier and ongoing training. BEHAVIOUR CHALLENGE BEHAVIOUR TO IMPROVE MOOD Figure 1: Cognitive Behavioural Model (CBM) RELAXATION EXERCISES CHALLENGE THINKING TO IMPROVE MOOD FEEL ANXIOUS + PHYSIOLOGICAL AROUSAL SOMETHING BAD WILL HAPPEN & I WON’T BE ABLE TO HANDLE IT STRESSFUL CLINICAL SITUATION Acknowledgements • Radha MacCulloch AVOIDANCE References CREATE AN ACTION PLAN TO IMPROVE MOOD Outcomes Figure 2: CBM applied to a stressful clinical encounter Beck AT. The Current State of Cognitive Therapy: a 40 year Retrospective.Arch Gen Psychiatry. 2005; 62(9):953-9. Beck R, Daughtridge and PD Sloane. Physician-Patient Communication in the Primary Care Office: A Systematic Review. J Am Board Fam Pract 2002;15:25-38. Frank JR. (Ed). 2005. The CanMEDS 2005 physician competency framework. Better standards. Better physicians. Better care. Ottawa: The Royal College of Physicians and Surgeons of Canada Skeff KM, Stratos GA, Bergen MR. Evaluation of a Medical Faculty Development Program: A Comparison of Traditional Pre/Post and Retrospective Pre/Post Self- Assessment Ratings.Evaluation & The Health Professions 1992; 15(3):350-366. Supported by the Educational Development Fund THOUGHTS / ATTITUDES FEELINGS (of MD and of Patient / Parent) (of MD and of Patient / Parent) DIFFICULT COMMUNICATION TASK BEHAVIOUR NON-VERBAL COMMUNICATION (of MD and of Patient / Parent) Figure 3: CBM applied before / during / after clinical encounter