Download
1 / 15
190 likes | 688 Views
The Payment Control Knob. Peter Berman The World Bank AFR Flagship Course on Health System Strengthening Kigali, Rwanda June 28, 2010. From Control Knobs to Outcomes. The Payment Control Knob.

E N D
The Payment Control Knob Peter Berman The World Bank AFR Flagship Course on Health System Strengthening Kigali, Rwanda June 28, 2010
The Payment Control Knob • Like other CKs – comprises a domain of policy action – the payment and purchasing actions in the health system -- which can be adjusted to affect health system performance • Payment focuses our attention on the pecuniary or financial incentives – a powerful tool for changing organizational, provider, and consumer behavior (one of the main contributions of health economics) • Financial incentives are important, but they are not all powerful. Their effect depends as well on other things, including organizational factors and other determinants of motivation and behavior
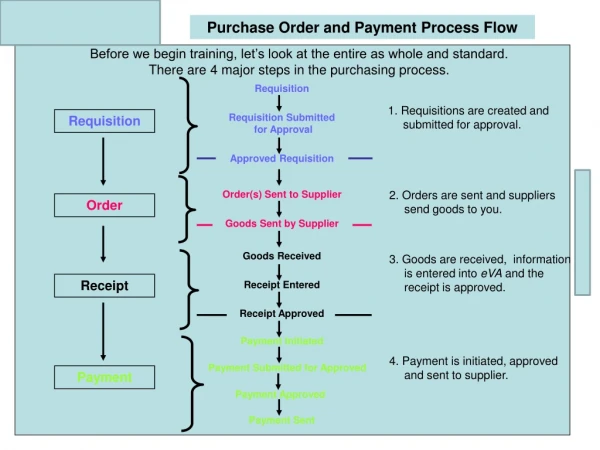
How payment works • Payment strategies are present at different levels • Each purchasing institution e.g. insurance fund, local govt; • Government system-level policies can directly and indirectly change purchasers’ behavior • Payment operates through 2 mechanisms: • Direct incentives on organizations and providers • Distribution of financial risk • Different payment methods include BOTH incentive aspects and risk aspects – and you need to understand both • Plus – different methods make different demands on administration and management – some are easier and less costly to use • You need to find “the right tool for the job”
Key dimensions of payment methods • Who is being paid: organization, individual provider • Who is making the payment: purchaser, patient, community • What is the unit for which payment is being made? • How much is being paid for each unit? • When is the payment level determined and when is payment made? How does this affect the risks to the payer, the provider, the patient? • For provider…In advance of the service rendered? Prospective • For provider…After the service has been rendered? Retrospective • For patient…After the patient has paid for the service? Reimbursement • For patient…Part of cost after the patient has received the service? Copayment and deductible
A simple truth and some complexity • Providers respond to financial incentives in payment (as do professors and WB economists) • But – it does not follow that this response is always very large or that it is worth the financial and social cost
Norms, exceptions, and innovations • Most government health care delivery systems rely on salary and budget payment methods in LICs. This is MUCH less the case in MICs and HICs. • Even in salary and budget paid systems, there are often exceptions for specific programs and areas, such as specific disease control programs and more remote or more costly areas. • New PBF initiatives reflect increasing interest in broader innovations to use payment incentives
Study Aims • Evaluation of payments to 3 hospitals for inpatient and outpatient services • Each hospital purchased its own medicines and set its own service charges • Each hospital faces multiple payment sources, resulting in different prescribing and dispensing guidelines
Small group discussion (6 groups at tables) • For your country or a country you know • Identify examples of 2 different payment methods being used in the government system which you think WORK WELL, i.e. providers do their jobs, decent service is delivered, patients are relatively satisfied • Briefly describe the characteristics of the payment method we have discussed • Explain why you think it works well, with reference to incentives and motivation, who bears risk, administrative complexity • Report back briefly (<5 minutes per group)