Download
1 / 20
• 200 likes • 215 Views
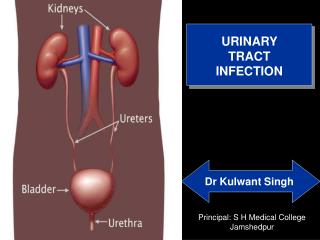
“Imaging Studies after a First Febrile Urinary Tract Infection in Young Children”. Brent Lee Lechner, D.O. MAJ, MC, USA. Background. American Academy of Pediatrics Practice Guidelines 1 st Urinary Tract Infection(UTI) in a 2-24 month old Voiding Cystourethrogram (VCUG) Renal Ultrasound

E N D
“Imaging Studies after a First Febrile Urinary Tract Infection in Young Children” Brent Lee Lechner, D.O. MAJ, MC, USA
Background • American Academy of Pediatrics Practice Guidelines • 1st Urinary Tract Infection(UTI) in a 2-24 month old • Voiding Cystourethrogram (VCUG) • Renal Ultrasound • Although these imaging studies performed routinely, little evidence to support their use to improve outcome
Objective • Assess the value of routine imaging studies after the diagnosis of a first febrile UTI in children 1 to 24 months
Multicenter, Randomized Clinical Trial Initial Study: evaluate the efficacy of oral vs IV therapy in children with fever Years: 1992-1997 Written Informed Consent obtained from parents Urine cultures obtained at 3 and 6 months or febrile illness Duration of follow-up: 6 months Eligible Children Age: 1-24 months old Fever to 38oC (rectal temp) UTI suspected if: Pyuria (10 or > WBC/hpf) Bacteria (1 or > Gram- rods on Gram Stain) Final Criteria Positive Urine Culture Greater than 50,000 colony-forming units on catheter urine Study Design
Treatment • Two Groups • Group One (Hospitalized Group): • Intravenous Cefotaxime (200mg/kg/d) q6h X 3days • Cefixime (8mg/kg/d) qd for 14 days • Group Two (Outpatient): • Oral Cefixime (16 mg/kg/1st dose in ER), then (8 mg/kg/d) qd for 14 days • Both Groups received antibiotic prophylaxis with Cefixime (4mg/kg/d) for 11 months or until a VCUG obtained
Imaging Studies • Three Studies Evaluated • Renal Ultrasound: • within 48 hours of diagnosis to evaluate anatomy • Voiding Cystourethrogram (VCUG): • 1 month after diagnosis to evaluate vesicoureteral reflux (VUR) • Technetium-99m-labeled dimercatosuccinic acid (DMSA): • 48 hours of diagnosis to evaluate pyelonephritis • 6 months later to evaluate renal scarring
Vesicoureteral Reflux (VUR) • Grade I - Reflux in Ureter • Grade II - Reflux to the Upper Collecting System, No dilation • Grade III - Reflux into dilated ureter and/or blunted calyces • Grade IV - Grossly dilated ureter • Grade V - Tortuosity
Dimercaptosuccinic Acid scintigraphy(DMSA) • 99M Tc-DMSA bound to renal tubular cells • DMSA gives image of functional tubular mass • Acute Pyelonephritis • Decreased uptake • No cortical loss • Scarring • Cortical loss and/or contour of kidney loss
Initial Imaging Studies • 421 Children (1-24 months) enrolled • 23 No parental consent • 76 Not enrolled (previous abx, language barrier, PCP refusal, etc.) • 13 Abnormal Urinanalysis but negative Urine Culture • Total: 309 (276 girls and 33 boys) enrolled
Initial Imaging Studies • All 309 children had a renal ultrasound and DMSA scan • 272 (88 percent) had normal Renal US • 190 (61 Percent) had findings that fit definition of acute pyelonephritis on DMSA • 1 Child had evidence of previous scarring • Mean Percentage of renal parenchymal involvement in acute pyelonephritis • 31 percent
Follow-up Imaging Studies • VCUG • 302 of 309 children had VCUG (98 percent) • 185 of 302 Normal VCUG (61.3 percent) • 117 of 302 Evidence of VUR (39 percent) • 112 of 117 Grade I,II,III (96 percent)
Evidence of Dilation based on Grade of VUR • Renal Ultrasound with dilation • VUR: 12 of 30 (40%) • Renal Ultrasound without dilation • VUR: 105 of 272 (39%) • Abnormal Ultrasound seen with Grade III or IV VUR • VUR Grade III or IV: 10 of 30 (33%) • Normal Finding: 40 of 272 (15%)
DMSA Scan Results • Repeated DMSA scan done in 275 of 309 • 89 % of patients at six months • Small Renal Parenchymal Involvement (8.2%) • 26 of 275 (9.5%) • Acute Pyelonephritis • 26 of 173 (15%) • Renal Scarring VUR vs No VUR • VUR: 16 of 109 (15%) • No VUR: 10 of 166 (6%)
Discussion • Large Number of Children for Pediatric Study • Study focused on 1st time Febrile UTI • Renal US not helpful in identifying Grade I,II or III • Grade IV VUR • Very Small number though • Renal US is not helpful in clinical management decisions • Most urinary obstruction is seen in the prenatal period • 309 children did not have obstruction • No recommendation for routine renal US
Discussion • Antibiotic Prophylactic therapy based on premise that children with acute pyelonephritis and VUR leads to scarring • Corrects spontaneously or surgically • Does the reflux or infection cause the scarring? • Need a placebo versus prophylactic antibiotic group study to assess scarring • Until new study, VCUG is warranted and remains warranted even if scarring caused by reflux
Discussion • DMSA scan in the acute phase indicates acute pyelonephritis but does not alter treatment • In children with febrile UTI, 60-65% will be positive on DMSA for kidney involvement • No recommendation for DMSA scan • Previous Studies indicate 30% renal scarring • This study is 9.5% • Definition of Renal Scarring is the question • This study shows small scars
Summary • Renal US and DMSA scan limited value at the time of acute 1st time UTI • No change in management • VCUG is recommended • No data concerning renal damage from reflux • Rather than frequent DMSA at six month intervals, strong commitment to UA and urine culture in subsequent febrile illness in all children with previous febrile UTI can obviate need.