Download
1 / 22
220 likes | 894 Views
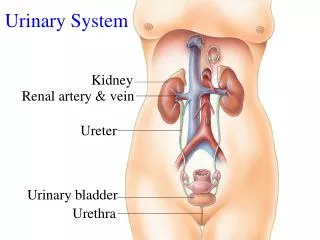
Urinary tract Infaction UTI means infection of any part of urinary tract (Kidney, Ureter, Bladder or Urethra) Defined by the presence of more than a hundred thousand organisms per ml in midstream sample of urine. Common organisms :

E N D
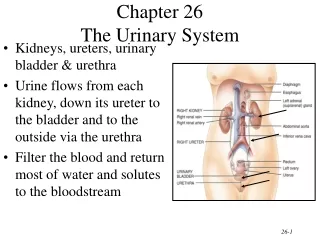
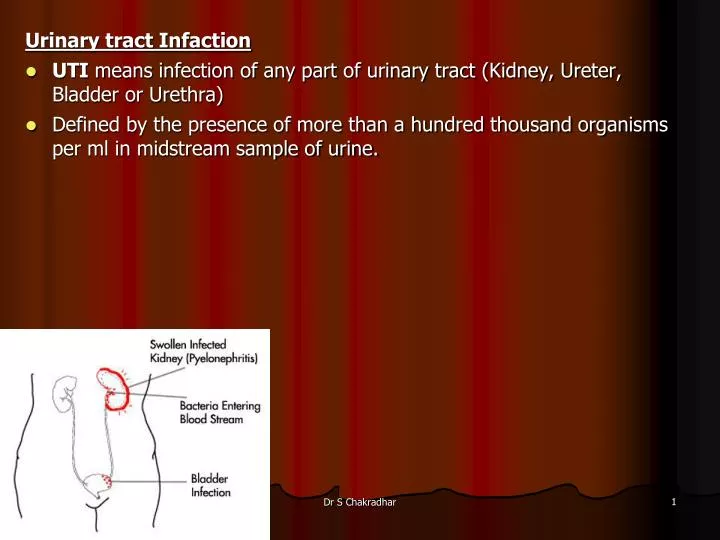
Urinary tract Infaction • UTI means infection of any part of urinary tract (Kidney, Ureter, Bladder or Urethra) • Defined by the presence of more than a hundred thousand organisms per ml in midstream sample of urine. Dr S Chakradhar
Common organisms : • E. coli, proteus , pseudomonas, klebsiella , Enterococcus fecalis , Staphylococcus saprophyticus or Staph epidermidis Predisposing condition • Urinary obstruction • Pregnancy • Vesicouretic reflux • Sex & age – Common in female between 1st year to 40 years of age • Common in male in advanced age due to prostatic hypertrophy • Diabetes mellitus • Immunosuppression & immunodeficiency • Instrumentation like cauterization Dr S Chakradhar
Routes of spreads : • Ascending transurethral route • From the lower UT is the commonest • At first there is colonisation of the distal urethra & introitus in female by coliformbacteria • Hematogenous • Through blood stream e.g. septicaemia • Lymphatics • Direct extension from vesico colic fistula Dr S Chakradhar
Classification • Lower urinary tract infection (Urethritis, Cystitis, Prostatitis) • Upper urinary tract (Pyelonephritis) Complicated UTI • Is considered to be present when there are underlying factors that predispose to ascending bacterial infection. Uncomplicated UTI • Occurs without underlying abnormality or impairment of urine flow. Dr S Chakradhar
Clinical features: • Fever, rigor. Vomiting • Increased frequency, urgency, dysuria (scalding pain during passage of urine ) • Intense desire to pass more urine • Suprapubic pain during and after micturation in case of cystitis. • Urine may be cloudy. Sometimes gross hematuria. • There may be slight or no systemic disturbance. Dr S Chakradhar
Investigation: • TC, DC, ESR, Hb • Urine culture and sensitivity • Culture suggesting>100,000 of the same organism/ml indicate UTI. • IVU, micturating urethrography • USG • Cystoscopy Dr S Chakradhar
Management • Maintain good urine flow by increasing fluid intake. • Appropriate Antibiotics : Ciprofloxacin, Coamoxyclav, Norfloxacin, Cephalosporins are commonly used. • For uncomplicated treatment is given for 3 days and for complicated 7-14 days. • Potassium citrate mixture 10ml in a glass of water three times a day, It alkalinizes the urine and relieves dysuria. • If severe symptoms bladder relaxants (Flavoxate 200 mg TID) can be used. Dr S Chakradhar
Prophylactic measures • Plenty of fluid intake • Frequent emptying of bladder • Double micturation at bed time • Emptying bladder before & after intercourse • Application of 0.5% cetrimide cream to preurethral area before intercourse • Urine culture should be repeated after treatment Dr S Chakradhar
UPPER URINARY TRACT INFECTION Dr S Chakradhar
ACUTE PYELONEPHRITIS It is characterized by an acute inflammation of the parenchyma & pelvis of the kidney. Pathology • Usually enlarged due inflammatory PMNs and edema. • Infection is focal and patchy, beginning in the pelvis, medulla and extending into the cortex Dr S Chakradhar
Clinical features • Sudden onset pain in both loins radiating to iliac fossae and suprapubic area. • Urinary symptoms like frequency and dysuria • Fever is usually present. It may be associated with chills, rigor, and vomiting. • Tenderness in the renal angle and lumbar region. Dr S Chakradhar
Investigation – look up UUTI Management • Ciprofloxacin, Norfloxacin, Co-Amoxyclav are common drugs used. • Total duration of the therapy is 1-2 weeks. • Severe cases require IV therapy • General measures – same as lower UTI Dr S Chakradhar
Complications: • Chronic Pyelonephritis • Sepsis and shock • Papillary necrosis particularly DM & UT obstruction it may lead to acute renal failure • Pyonephrosis – suppurativeexudate fills the renal pelvis calyces & ureter when there is total complete obstruction • Perinephric abscess – suppurative inflammation extends through the renal capsule into perinephric tissue D/D: • Acute Appendicitis • Salpingitis • Cholecystitis • Diverticulitis • Perinephric abscess. Dr S Chakradhar
Chronic Pyelonephritis • It may be unilateral or bilateral. It occurs in 2 forms Chronic Obstructive P • There is recurrent bouts of acute inflammation superimposed on diffuse or localized obstructive lesions – pregnancy Reflux associated pyelonephritis (reflux nephropathy) • It starts early in childhood. There is urinary infection on congenital vesicouretal reflux Dr S Chakradhar
Pathology: • Are usually scarred – asymmetry • Coarse, discrete corticomedullary scar overlying a blunted or deformed calyx Dr S Chakradhar
Clinical Features: • Recurrent attacks of Frequency, Dysuria, Aching Lumbar pain • Usually patient comes with Lassitude, Tiredness, Vague ill health, • Symptoms of uraemia • Arterial hypertension • Pyuria , Proteinuria Dr S Chakradhar
Investigations: Management • Antibiotics according to culture and sensitivity report • Usually Ciprofloxacin • Total duration : 3-6 months • Remove if there is presence of obstruction • Vesicoureteric reflux spontaneously disappears in adult life • General measures Dr S Chakradhar
RENAL TUBERCULOSIS • It is a consequence of miliary TB • Most heal, but in some, infection persists and spreads to the papillae, with the formation of cavitating lesions and the discharge of mycobacteria into the urine. • Infection of the ureters and bladder commonly follows, with the potential for the development of ureteral stricture and a contracted bladder. Dr S Chakradhar
Clinical Features • Typical features of TB • Frequency of micturation & Dysuria, • Hematuria, pyuria Investigation • TC, DC, ESR, Hb • Cystoscopy • Urine RME • Culture of acid-fast bacilli from early morning urine specimens • Chest X ray, mantoux test • Excretory urography, USG • Renal biopsy. Treatment • ATT with steroid Dr S Chakradhar
Excretory urography in a patient with renal tuberculosis shows an irregular cavity at the upper pole calyx of the right kidney. Note the multiple tiny calcifications in the liver, spleen, and right adrenal gland due to calcified tuberculous granuloma. Dr S Chakradhar
Lobar calcification in a large destroyed right kidney in a patient with renal tuberculosis. Note the involvement of the right ureter. Dr S Chakradhar