Download
1 / 87
870 likes | 1.04k Views
STIs in Pregnancy. Lisa M. Hollier, MD, MPH University of Texas Houston Medical School. Conflicts of Interest.

E N D
STIs in Pregnancy Lisa M. Hollier, MD, MPH University of Texas Houston Medical School
Conflicts of Interest • According to ACCME policy, the speakers must disclose all associations with proprietary entities that may have a direct relationship to the subject matter of this lecture. They must also disclose any discussion of unlabeled or unapproved uses of products.
Conflicts of Interest • I have no such financial relationships • I will not discuss unlabeled or unapproved uses of products.
Educational Objectives This lecture should enable you to: • Be familiar with the epidemiology of STIs in pregnancy • Know who and how to screen for infection • Compare and contrast various treatment options
Sexually Transmitted Infections • STIs are a major public health challenge in the United States • CDC estimates that 19 million new infections occur each year, almost half of them among young people ages 15 to 24 • Direct medical costs associated with STDs in the US are estimated at up to $14.1 billion annually CDC Surveillance Report 2005
Chlamydia Epidemiology CDC STD Surveillance Report 2007
Chlamydia in Pregnancy • About 10% of patients screen positive • Complications controversial • preterm delivery • premature rupture of membranes • postpartum infection
Chlamydia in Pregnancy • Neonatal infections: • Pneumonia • Conjunctivitis • 60-70% of exposed infants become infected
Diagnosis • Non-amplified tests • Nucleic Acid Hybridization (NA Probe), e.g. Gen-Probe Pace-2 • sensitivities ranging from 75% to 100%; specificities greater than 95% • detects chlamydial ribosomal RNA • able to detect gonorrhea and chlamydia from one swab • need for large amounts of sample DNA
Diagnosis • DNA amplification assays (NAATs) • polymerase chain reaction (PCR) • ligase chain reaction (LCR) • transcription-mediated amplification (TMA) • strand displacement amplification (SDA) • Sensitivities with PCR and LCR 95% and 85-98% respectively; specificity approaches 100%
Diagnosis • PCR testing of self-collected samples from the vaginal introitus yielded sensitivities/specificities similar to physician-collected samples Ostergaard L. BMJ 1996;313(7066):1186-9
Treatment • Recommended regimens • Azithromycin 1 gm single dose or • Amoxicillin 500mg po TID x 7 days CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
Treatment • Alternative regimens • Erythromycin base 500 mg qid for 7d • Erythromycin base 250 mg qid for 14d • Erythromycin ethylsuccinate 800 mg qid for 7 days • Erythromycin ethylsuccinate 800 mg qid for 14 days CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
“Test of Cure” • Recommended for all pregnant women: • Repeat testing (preferably by NAAT) 3 weeks after completion of therapy to ensure therapeutic cure • Important sequelae might occur in the mother and neonate if the infection persists CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
Partner Mgmt • Instruct patients to refer their sex partners for evaluation, testing, and treatment • Most recent partner • Any partner within last 60 days • If partner evaluation/treatment unlikely • Consider delivery of antibiotic therapy by patients to their partner • Limited studies demonstrate trend toward a decrease in persistent or recurrent chlamydia CDC. STD Treatment Guidelines. MMWR 2006;55(No. RR-11)
Infant Treatment • Infants born to mothers who have untreated Chlamydial infection • high risk for infection • prophylatic antibiotic treatment is not indicated • infants should be monitored to ensure appropriate treatment if symptoms develop CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
Controversies • When to screen • Who to screen
Gonorrhea Epidemiology CDC STD Surveillance Report 2007
Gonorrhea in Pregnancy • Complications more common in women with infection • septic spontaneous ab & postabortal infection • preterm delivery • premature rupture of membranes • chorioamnionitis • postpartum infection
Gonorrhea in Pregnancy • Neonatal infections: • ophthalmia neonatorum • scalp abscess • disseminated disease
Disseminated Infection • Gonococcal bacteremia • may lead to petechial or pustular skin lesions, arthralgias, septic arthritis, or tenosynovitis • Pregnant women may account for disproportionate number of cases • may include fatal endocarditis
Diagnosis • Non-amplified DNA probe tests • Nucleic acid amplification tests • PCR, TMA • High false positive rate for Amplicor PCR—consider repeating positive tests with different assay • If culture is done use dacron or rayon swab with modified Thayer-Martin media
Diagnosis • Use of NAAT for rectal and oropharyngeal specimens is being evaluated • Traditional culture may be used in these situations
Treatment • Recommended regimens • Ceftriaxone 125mg IM or • Cefixime 400mg po • Alternative regimen • Spectinomycin 2gm IM CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
Syphilis • Rates in US fell until 2000: < 8,000 cases • Cases are rising in men over the last 3 years • Incidence highly concentrated • Half of all US cases in 22 cities and counties • mostly in the South, among poor blacks and Hispanics CDC Surveillance Report 2007
Syphilis • Total rate of primary and secondary syphilis: 3.8 per 100,000 population • Congenital syphilis 10.5 per 100,000 live births CDC Surveillance Report 2007
Syphilis in Pregnancy • Complications • spontaneous abortion • preterm birth • fetal death • congenital infection by transplacental or perinatal transmission
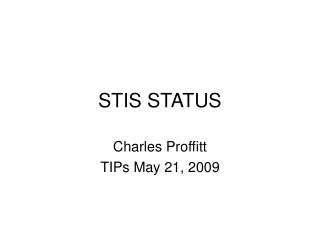
Secondary syphilis • Rash is usually symmetric and dry • Flaky nodular lesions are most common Source: Tania Lee, MD
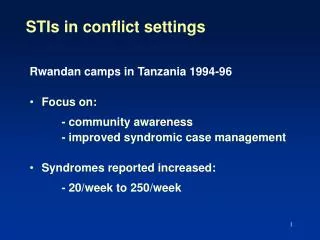
Secondary Syphilis Condylomata Lata Smooth, raised areas that are teaming with spirochetes Source: Tania Lee, MD
Diagnosis • Screening with nonspecific test • Rapid plasma reagin (RPR) • Venereal Disease Research Laboratory (VDRL) • Automated Reagin Tests • Generally quantitative • Very sensitive
Diagnosis • Confirmation with a Treponemal specific test • Fluorescent treponemal antibody absorbed (FTA-ABS) • Treponema pallidum particle agglutination test (TP-PA)
Treatment • Obtain treatment history from health department • Benzathine Penicillin G 2.4 million units IM • One injection for primary syphilis • One or two injections for secondary and early latent • Three injections one week apart for late latent or unknown duration • Desensitize if PCN-allergic CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
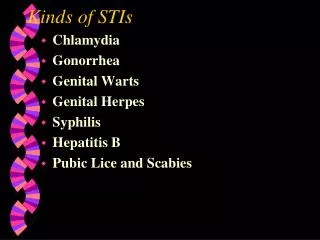
Efficacy of Syphilotherapy by Stage Alexander JM et al.Obstet Gynecol 1999; 93:5-8
Treatment • Because of reports of treatment failure with azithromycin, penicillin is the preferred therapy. • 2-gram dose of azithromycin may be considered for penicillin-allergic patients, but only with close follow-up because treatment efficacy is not well documented and has not been studied in persons with HIV infection CDC. MMWR 2004;53(09);197-198
Treatment • Some experts recommend ultrasound prior to syphilotherapy in pregnancy CDC. Sexually Transmitted Diseases Treatment Guidelines. MMWR 2006;55(No. RR-11)
Congenital Syphilis • Ultrasound findings • Hepatomegaly • Polyhydramnios • Placentomegaly • Ascites • Hydrops
Follow-up • Notify health department of treatment • Serofast • RPR each trimester • Primary or Secondary • At least every trimester (?monthly) • Latent syphilis • At least every trimester
Controversies • Testing with EIA • Penicillin allergy testing • Use of MCA doppler for fetal assessment
Hepatitis B • 350 million chronically infected patients worldwide • Perinatal transmission accounts for 35-50% of hepatitis B carriers • 70-90% of infants born to positive women will be chronically infected • Risk of perinatal transmission closely related to HBeAg status
Hepatitis B in Pregnancy • Approximately 25% of the frequent sexual contacts of infected individuals will themselves become infected • Serologic testing and possible vaccination of sexual partner and household contacts should be discussed
Hepatitis B in Pregnancy • Serologic testing • HepBsAg positive • Confirm chronic infection • Presence of Heb B core IgG • Absence of Hep B core IgM • Liver function tests • HIV • HepBeAg, if available
Hepatitis B in Pregnancy • Risk of hepatitis B infection through amniocentesis is low • Knowledge of hepatitis Be antigen status may be valuable in counseling about risks Davies G et al. J Obstet Gynaecol Can 2003;25:145-48