Download
1 / 35
360 likes | 393 Views
Learn about Clostridium bacteria, anaerobic conditions, oxygen detoxification, and diseases caused by Clostridium species like tetanus. Explore their shapes, physiology, toxins, transmission, and clinical findings.

E N D
Clostridium spp Part I Dr. Wasan Abdul-ilah Bakir
Anaerobic Bacteria • Bacteria are often categorized according to their growth responses to atmospheric oxygen. This may vary from species that can grow only in the presence of oxygen to those that can grow only in the absence of oxygen.
Anaerobic Bacteria • Bacteria that require anaerobic conditions to initiate and sustain growth. • Bacteria can exist in a wide variety of environments, including environments that lack oxygen. • In fact, oxygen is toxic to some bacteria. This toxicity is usually due to the accidental formation of superoxides (O2-) and hydrogen peroxide (H2O2), which react with other cell components. • Oxygen is harmful if : • Oxygen concentration is very high in media or air. • Bacteria have no enzyme system to eliminate it.
Anaerobic Bacteria Oxygen Detoxification • Toxic forms of oxygen need to be neutralized by Enzyme systems. • Superoxide dismutase • Catalase • Peroxidase • If microbe does not produce these enzymes, must have anaerobic conditions. • Cells that live in oxygen-containing environments have the enzymes superoxide dismutase and catalase (among others) that convert superoxides and peroxides to oxygen and water.
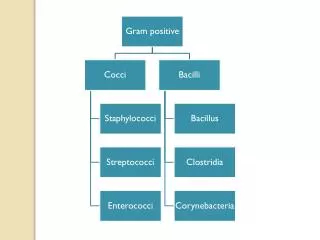
Clostridium • Characteristics • Gram-positive . • obligate anaerobes • capable of producing endospores which protect them in harmful environment . • Individual cells are rod shaped. • The spores are usually wider than the rods, and are located terminally or sub terminally. • Most clostridia are motile by peritrichous flagella while others have a capsule like Clostridium perfringens
Most Common Clostridium Species • The clostridia consist of many species that include common free-living bacteria as well as important pathogens. • Many decompose proteins or form toxins, and some do both. Their natural habitat is the soil, marine sediments, sewage, or the intestinal tract of animals and humans, where they live as saprophytes. * They cause disease primarily through the production of numerous exotoxins. • There are four main species responsible for disease in humans:. C. tetani: tetanus C. botulinum: botulism C. perfringens: gas gangrene; food poisoning C. difficile: pseudomembranous colitis
Shapes Of Clostridia The shape an position of spores varies in different species and is useful the identification of Clostridia *Central in Cl. bifermentans *Sub terminal in Cl. perfringens *Oval and terminalin Cl. tertium *Spherical and terminal giving drum stickappearancein Cl. tetani
Clostridium tetani Physiology and Structure - Anaerobic bacteria , it is gram positive, slender bacillus and it has spherical terminal spores giving drum stick appearance -It is non capsulated - motile with peritrichus flagella. -It produces a potent biological toxin, tetanospasmin, and is the causative agent of tetanus a disease characterized by painful muscular spasms that can lead to respiratory failure.death.
What is Tetanus? • An infectious disease caused by contamination of wounds from the bacteria Clostridium tetani, or the spores they produce that live in the soil, and animal feces. • Infection follows when spores • become activated and develop • into gram-positive bacteria that multiply • and produce a very powerful toxin (tetanospasmin) that affects the muscles.
Transmission • Tetanus spores are found throughout the environment, usually in soil, dust, and animal waste. • Tetanus is acquired through contact with the environment.
Transmission • The usual locations for the bacteria to enter the body: • Puncture wounds (such as those caused by rusty nails, splinters, or insect bites). • Burns, any break in the skin, and IV drug access sites are also potential entryways for the bacteria.
C. tetani Pathogenesis C. tetani is not an invasive organism. The infection remains localized in the area of devitalized tissue (wound, burn, injury, umbilical stump, surgical suture) into which the spores have been introduced. The volume of infected tissue is small, and the disease is almost entirely a toxemia. Germination of the spore and development of vegetative organisms that produce toxin are aided by: (1) necrotic tissue (2) calcium salts (3) associated pyogenic infections, all of which aid establishment of low oxidation-reduction potential.
C. tetani Toxin The toxin (tetanospasmin) released from vegetative cells reaches the central nervous system by retrograde axonal transport or via the bloodstream rapidly becomes is bind to ganglioside receptors blocks release of inhibitory mediators ( glycine and γ aminobutyric acid ( GABA) at spinal synapses. Hyperreflexia, muscle spasms, and spastic paralysis result.
C. tetani Toxin Tetanospasmin is responsible for clinical manifestations of tetanus. • Tetanospasmin blocks GABA • Cause intense muscle spasm (causing spastic paralysis).
C. tetani Clinical Finding Tetanus is characterized by strong muscle spasms (spastic paralysis, tetany). The incubation period may range from 4 to 5 days up to 3 weeks. Muscular spasms often involve first the area of injury and infection and then the muscles of the jaw (trismus, lockjaw), which contract so that the mouth cannot be opened. Any external stimulus may precipitate a tetanic generalized muscle spasm. In advanced disease patients rigid in moderate opisthotonos with arm extended, abdomen boardlike and respiratory failure ensues. A high mortality rate is associated with this disease. Note that tetanus, spastic paralysis (strong muscle contractions) occurs, whereas in botulism, flaccid paralysis (weak or absent muscle contractions) occurs
C. tetani Laboratory Diagnosis Diagnosis depends on the clinical picture and a history of injury. Anaerobic culture of tissues from contaminated wounds may yield C tetani depends on production of toxin and its neutralization by specific antitoxin. • Anaerobic culture of tissues from contaminated wounds may yield C. tetani . • Inoculation of culture in to 2 mice one is protected with anti-toxin and the other is unprotected (dies with typical tetanic spasms )
C. tetani Prevention, Treatment 3.Prophylactic use of antitoxin. The DTaP vaccine includes tetanus, diphteria and pertussis toxoids; it is routinely given in during childhood. After 7 years of age, only Td needs to be administered. Because the antitoxin levels decrease over time. 4.Antibiotic treatment. *Patients with symptoms of tetanus should receive muscle relaxants, sedation and assisted ventilation. • Prevention is much more important than treatment: • Active immunization with toxoid. • ‘Booster shot’ for previously immunized individuals. This may be accompanied by antitoxin injected into a different area of the body. • 2.Proper care of wounds. Surgical débridement to remove the necrotic tissue.
Penicillin strongly inhibits the growth of C tetani and stops further toxin production. Antibiotics may also control associated pyogenic infection.
C. botulinum Physiology and Structure C botulinum, which causes the disease botulism, is worldwide in distribution; it is found in soil and occasionally in animal feces. Types of C botulinum are distinguished by the antigenic type of toxin they produce. Spores of the organism are highly resistant to heat, withstanding 100°C for several hours. Heat resistance is diminished at acid pH or high salt concentration. .
C. botulinum Toxins During the growth of C botulinum and during autolysis of the bacteria, toxin is liberated into environment. Seven antigenic varieties of toxin (A-G) are known. Type A, B, E, and F are the cause of human disease(Botulinum toxin). Types A and B, have been associated with a variety of foods and type E with fish products. C botulinum toxins are among the most toxic substances known: The lethal dose for a human is probably about 1–2 µg/kg. The toxins are destroyed by heating for 20 minutes at 100°C.
C. botulinum Pathogenicity Botulinum toxin is absorbed from the gut carried via the blood, binds to receptors of presynaptic membranes of motor neurons of peripheral nervous system and cranial nerves where it blocks release of acetylcholine. It is a protease that cleaves the proteins involved in acetylcholine release. Along with tetanus toxin, it is among the most toxic substances known.
C. botulinum Transmission Transmitted by three ways: 1- Food or water toxin contamination 2- wound infected with C. botulinum 3-Ingestion of C. botulinum. Most common contaminated foods are: canned or vacuum-packed without adequate sterilization, spores survive and germinate in the anaerobic environment. Toxin is produced within the canned food and ingested preformed.
C. botulinum • The highest-risk foods are: • vegetables such as green beans, peppers, and mushrooms. • (2) smoked fish. • The toxin is relatively heat-labile; it is inactivated by boiling for several minutes. • Thus, disease can be prevented by sufficient cooking.
C. botulinum • Clinical Diseases • Foodborne botulism • Incubation period: 18-24 hrs. • Symptoms: double vision, • inability to swallow, speech difficulty, • bulbar paralysis, constipation, and abdominal pain. Bilateral descending weakness of peripheral muscle. Death occurs from respiratory paralysis or cardiac arrest. No fever. Mortality is high. • Patients who recover do not develop antitoxin.
C. botulinum • Clinical Diseases • Infant botulism • Occurs in the first month of life, when the infant ingest the spores germinate within the intestinal tract and produce toxin as they multiply, the neurotoxin then gets absorbed into the bloodstream. • Ingestion of honey containing the organism is implicated in transmission of infant botulism. • Affected infants develop weakness or paralysis and may need • respiratory support but usually recover.
C. botulinum • Wound botulism • in which spores contaminate a wound, germinate, and produce toxin at the site • Symptoms similar to those of food borne botulism with longer incubation time. Less GI symptoms.
C. botulinum Laboratory Diagnosis Culture of C. botulinum in patient feces and implicated food, but usually not cultured. Detection of toxin and not organism is required for definitive diagnosis. Toxin can be demonstrated in serum, gastric secretions or stool from the patient and in leftover food. swabs or other specimens obtained from patients should be transported using anaerobe containers. Suspect foods should be left in their original containers. Mice injected intraperitoneally with such specimens from these patients die rapidly. This mouse bioassay is the test of choice for the confirmation of botulism. Other methods used to detect toxin include ELISAs and PCR.
C. botulinum Treatment Stomach lavage and high enemas. Trivalent (A, B, E) antitoxin administered intravenously promptly, along with respiratory support. Adequate ventilation by mechanical respirator. Although most infant with botulism recover with supportive care alone, treatment with human – derived botulinum immune globulin (BIG)is recommended.
C. botulinum Prevention and Control Because spores of C botulinum are widely distributed in soil, they often contaminate vegetables, fruits, and other materials. When such foods are canned or otherwise preserved, they either must be sufficiently heated to ensure destruction of spores or must be boiled for 20 minutes before consumption. Toxic foods may be spoiled and rancid, and cans may “swell,” or the appearance may be innocuous. The risk from home-canned foods can be reduced if the food is boiled for more than 20 minutes before consumption.