Download
1 / 61
610 likes | 738 Views
Chapter 2. Principles and Methods of Drug Administration. Medication Administration. Nursing Responsibilities - Standard precautions - Patient privacy - Patient preparation - Drug preparation. Nursing Implications Associated with Drug Administration.

E N D
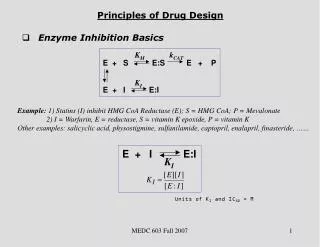
Chapter 2 Principles and Methods of Drug Administration
Medication Administration • Nursing Responsibilities - Standard precautions - Patient privacy - Patient preparation - Drug preparation
Nursing Implications Associated with Drug Administration • Consult references/pharmacist • Observe for ADR’s • Report drug reactions • Record observations • Withhold drug if needed - notify provider
Medication Orders • The nurse must ensure the patient receives the correct medication • Orders should include the following: • Name Date/time Drug name Dose Route Time/frequency administration Prescriber’s signature
Medication Orders • Controlled substances - Opioids, barbiturates, ect. double-locked - Keys with charge nurse - Log administration of drugs - End-of-shift count - Waste controlled substance with witness
Medication Orders • Types of orders - Standing orders - pre-written, no call - Verbal orders - telephone to nurse - repeat back to provider - To be written and signed by the provider asap
The Seven Rights of Medication Administration • Right drug • Right dose • Right patient: name and birth date • Right time • Right route • Right documentation • Patient’s right to refuse
Medication Preparation • Know the seven rights • Drug reference available • Know drug action, contraindications, usual dosage, and side effects • Check label 3 times - removing drug from container or drawer - on comparison with MAR - before giving to patient (if unit dose) - Before returning to drawer (if multi-use container)
Important Considerations • Enlist the patients • Utilize the pharmacists • Prepare one patient’s medication at a time • Minimize need for calculations or compare answers with another nurse’s • Two licensed nurses must double check high alert drugs before administration, i.e. insulin, heparin
Important Considerations • Always report errors • Never give an unlabeled drug • Don’t confuse drug names • Date and initial (multiuse vials or containers) • If you didn’t prep it, don’t give it
Important Considerations for Medication Administration • 2 identifiers for safety: name and DOB • If you gave it, chart it • Do not chart for someone else or have someone else chart for you • Do not transport or accept a container that is not labelled • Do not put down an unlabeled syringe
Important Considerations for Medication Administration • Watch the patient take it and swallow it • Assess patient’s response • If a patient refuses a medication: • do not force it, chart it • If you elect to omit a dose based on your nursing judgment, let another nurse help make the decision. If medication is not given, document, “dose omitted because…” Report to the provider
Commonly Used Abbreviations • Review pages 48-56 • Joint Commission on Accreditation of Healthcare Organization (JCAHO) approved abbreviation list • institutional policy and list of used abbreviations
Routes of Administration • Enteral - Via the GI Tract - Powders - Pills - Tablets - Liquids or suspensions - Suppositories
Routes of Administration • Percutaneous - Through the skin or mucous membranes - Topical - Instillation - Inhalation
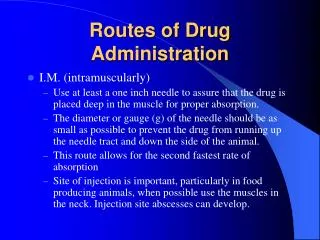
Routes of Administration • Parenteral - Methods other than the GI tract; needle route - Intramuscular (IM) - Subcutaneous (SC) - Intradermal - Intravenous (IV) - Ampules - Vials
Enteral Administration • Tablets, pills, capsules - absorbed more slowly from GI tract into the bloodstream than via any other route - (PO) route relatively safe - Do not crush enteric coated or sustained release pills - Only divide scored pills - Liquid medications: children and patients who cannot swallow pills
Oral Medications • Unit dosage system: most common • Med stays in package until administration • May place prepackaged medications in the same cup until administered • Involve the patient and include teaching • Patient refusal: return unopened medication to the drawer, document reason, notify provider
Oral Medications • From multi-dose containers, pour pill into the cap, drop into a medicine cup • Label cup with med name, dose • Do not touch meds with bare hands • Falls on floor? Toss it. Working on med cart? Add clean field
Enteral Administration of Liquid Medications • PO, or via a NG, gastrostomy, or jejunostomy tube • No liquids to unconscious patients: aspiration • Some liquid medications are not to be followed by water; some may stain the teeth • Use calibrated cup or syringe (but not IV syringe) • Measure liquids at bottom of meniscus
Enteral Administration of Tubal Medications • NG tubes: liquid meds to unconscious patients, dysphasic patients, those too ill to eat • Use liquid form or crush tablets and open capsules if allowed – give separately in warm water • Not all tablets are safe to use when crushed and not all capsules are safe to use when opened
Enteral Administration of Suppositories • Rectum or vagina • Dissolves at body temperature and absorbed directly into the bloodstream • infants, patients intolerant of oral preparations, N/V • Store in cool place
Administration of Vaginal Medications • Usually for yeast infections • Some products are used to induce labor • Use gloves • Provide privacy
Percutaneous Administration • skin /mucous membranes • Mostly local action; some act systemically • topical applications (ointments, creams, powders, lotions, and transdermal patches), instillations, and inhalations • Absorption is rapid, short duration
Percutaneous Administration • Ointments - oil-based; semisolid; skin or mucous membrane • Creams - Semisolid, non-greasy emulsions; external application • Lotions - Aqueous, soothing: pruritus, protectant, cleansing, astringent
Percutaneous Administration • Transdermal Patches Adhesive-backed, medicated patches -sustained, continuous release of medication over hours/days • Eye drops and Eye Ointments - Don’t touch the dropper or the tube to the eye (p 70 Fig 2-18) • Eardrops - ‘Otic’ solutions must be at room temperature when applied - Use only droppers supplied with medications for administration
Percutaneous Administration • Nose drops - individual use only • Nasal sprays - absorbed quickly; less medication used, wasted • Inhalations - mucous membranes ofrespiratory tract - relatively limited effect or a systemic effect - used by respiratory therapy and anesthesiologists
Percutaneous Administration • Sublingual medications - under the tongue, rapidly absorbed - tablet or a liquid squeezed from capsule - Do not give water after as water reduces absorption - tablet should dissolve (no swallowing) • Buccal medications - between the gum and the cheek, preferably above the molar - Follow same administration guidelines as SL
Parenteral Administration • Intramuscular (IM) • Subcutaneous • Intradermal • Intravenous (IV) • Rationale for using these methods include: - Absorption rate - No oral route - Emergencies - Drug is destroyed in the GI tract
Parenteral Administration • Equipment - Syringes - barrel, plunger, and tip - calibrated in milliliters, minims, insulin or heparin units - Types - Tuberculin syringe (for allergy testing/treatments, TB testing and small quantities) - Insulin syringe - One and three milliliter syringes - Safety-Lok syringes
Parts of a Syringe (From Elkin, M.K., Perry, A.G., Potter, P.A. [2004]. Nursing interventions and clinical skills. [3rd ed.]. St. Louis: Mosby.) .
Tuberculin Syringe Calibration (From Clayton, B.D., Stock, Y.N. [2004]. Basic pharmacology for nurses. [13th ed.]. St. Louis: Mosby.)
Calibration of U100 Insulin Syringe (From Clayton, B.D., Stock, Y.N. [2004]. Basic pharmacology for nurses. [13th ed.]. St. Louis: Mosby.)
Parenteral Administration • Equipment - Needles - Parts are the hub, shaft, and beveled tip - Opening at the needle’s beveled tip is the lumen - Size of the diameter of the inside of the needle’s shaft determines the gauge of the needle; the smaller the gauge, the larger the diameter - Needle gauge selection is based on the viscosity of the medication
Parts of a Needle (From Clayton, B.D., Stock, Y.N. [2004]. Basic pharmacology for nurses. [13th ed.]. St. Louis: Mosby.)
Parenteral Administration • Equipment - Needle length - Selected based on the depth of the tissue into which the medication is to be injected - Intradermal: 3/8 to 5/8 inch - Subcutaneous: ½ to 5/8 inch - Intramuscular: 1 to 1 ½ inch - Intravenous needles - Butterfly (scalp needle) - Over the needle catheter
Needle Length and Gauge (From Clayton, B.D., Stock, Y.N. [2004]. Basic pharmacology for nurses. [13th ed.]. St. Louis: Mosby.)
Parenteral Administration • Equipment - needleless devices - sheath or guard - IV caths: blunt-edged cannulas, valves, or needle guards - IV tubing: recessed and shielded needle connectors to reduce needle sticks
Parenteral Administration • Intramuscular (IM) injections - Site selection - Gluteal sites: ventrogluteal (gluteus medius) - Vastus lateralis muscle (thigh) - Rectus femoris muscle (thigh) - Deltoid muscle (arm) - Z-track method - Used to inject irritating meds
Locating IM Injection for Ventrogluteal Site (C, from Elkin, M.K., Perry, A.G., Potter, P.A. [2004]. Nursing interventions and clinical skills. [3rd ed.]. St. Louis: Mosby.)
Giving IM Injection in Vastus Lateralis Site on an Adult (C, from Elkin, M.K., Perry, A.G., Potter, P.A. [2004]. Nursing interventions and clinical skills. [3rd ed.]. St. Louis: Mosby.)
Rectus Femoris Muscle A. Child/Infant B. Adult (From Clayton, B.D., Stock, Y.N. [2004]. Basic pharmacology for nurses. [13th ed.]. St. Louis: Mosby.)
Giving IM Injection in Deltoid Site (C, from Elkin, M.K., Perry, A.G., Potter, P.A. [2004]. Nursing interventions and clinical skills. [3rd ed.]. St. Louis: Mosby.)
Figure 23-20 (From Potter, P.A., Perry, A.G. [2005]. Fundamentals of nursing. [6th ed.]. St. Louis: Mosby.) A, Z-track method. B, Using an air lock. C, Administering IM injection by airlock technique.
Parenteral Administration • Intradermal injections - serum, vaccine, or skin test agent - Not aspirated - Small volumes (0.1mL) injected to form a small wheal just under the skin - Used for allergy sensitivity tests, TB screening, local anesthetics - tuberculin syringe with 25-gauge, 3/8 to 5/8 inch needle
Figure 23-21 (From Potter, P.A., Perry, A.G. [2005]. Fundamentals of nursing. [6th ed.]. St. Louis: Mosby.) Angles of insertion for intramuscular (90°), subcutaneous (45°), and intradermal (15°).
Parenteral Administration • Subcutaneous injections - loose connective tissue between the dermis and the muscle layer (fatty layer) - absorption slower than with IM injections - Given at a 45-degree angle if the patient is thin or at a 90-degree angle if the patient has ample subcutaneous tissue - Usual needle length is ½ to 5/8 inch and 25 gauge - insulin and heparin
Subcutaneous Injection • Angle and needle length depend on the thickness of skin fold (From Elkin, M.K., Perry, A.G., Potter, P.A. [2004]. Nursing interventions and clinical skills. [3rd ed.]. St. Louis: Mosby.)