Download
1 / 1
10 likes | 121 Views
TREATMENT OF LARGE AND GIANT COLORECTAL POLYPS IN THE REAL WORLD . S. Husson, G. Ventre, F. Vagne, J.F. Vies, M. Musso, J.L. Colson, J. Picot, J.M. Boyaval, D. Sondag, F. Khachoyan, I. Gendre, P. Perrin, B. Denis.

E N D
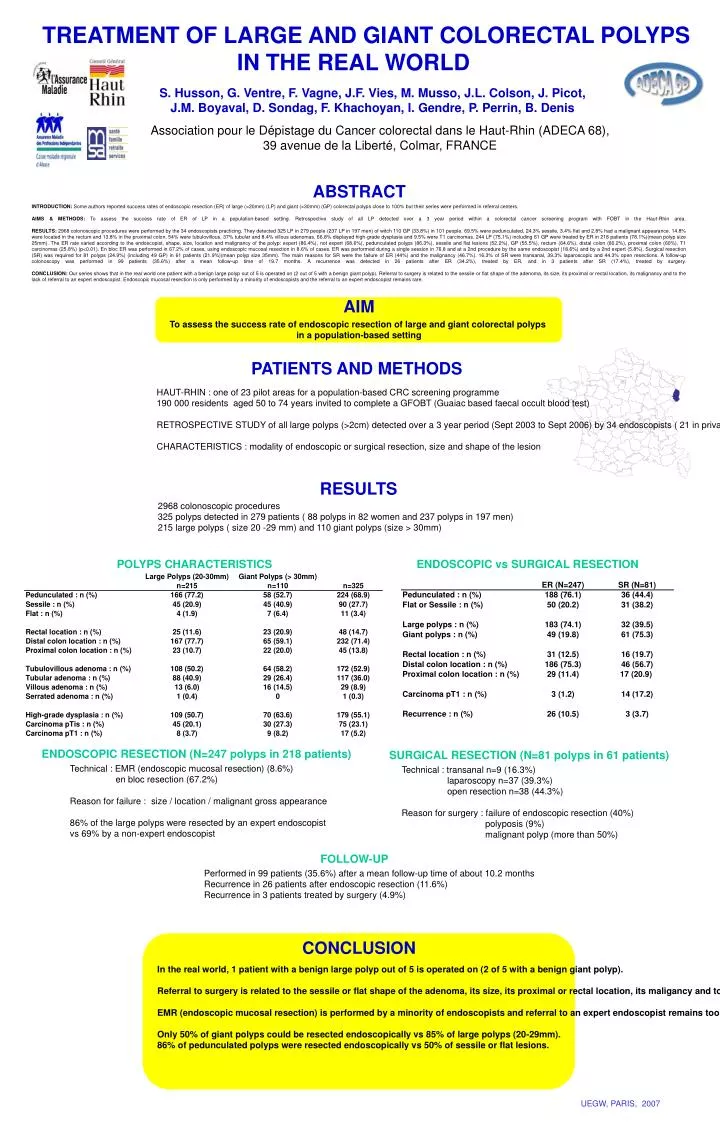
TREATMENT OF LARGE AND GIANT COLORECTAL POLYPS IN THE REAL WORLD S. Husson, G. Ventre, F. Vagne, J.F. Vies, M. Musso, J.L. Colson, J. Picot, J.M. Boyaval, D. Sondag, F. Khachoyan, I. Gendre, P. Perrin, B. Denis Association pour le Dépistage du Cancer colorectal dans le Haut-Rhin (ADECA 68), 39 avenue de la Liberté, Colmar, FRANCE ABSTRACT INTRODUCTION: Some authors reported success rates of endoscopic resection (ER) of large (>20mm) (LP) and giant (>30mm) (GP) colorectal polyps close to 100% but their series were performed in referral centers. AIMS & METHODS: To assess the success rate of ER of LP in a population-based setting. Retrospective study of all LP detected over a 3 year period within a colorectal cancer screening program with FOBT in the Haut-Rhin area. RESULTS: 2968 colonoscopic procedures were performed by the 34 endoscopists practicing. They detected 325 LP in 279 people (237 LP in 197 men) of witch 110 GP (33.8%) in 101 people. 69.5% were pedunculated, 24.3% sessile, 3.4% flat and 2.8% had a malignant appearance. 14.8% were located in the rectum and 13.8% in the proximal colon. 54% were tubulovillous, 37% tubular and 8.4% villous adenomas. 66.8% displayed high-grade dysplasia and 9.5% were T1 carcinomas. 244 LP (75.1%) including 61 GP were treated by ER in 218 patients (78.1%)(mean polyp size 25mm). The ER rate varied according to the endoscopist, shape, size, location and malignancy of the polyp: expert (86.4%), not expert (68.6%), pedunculated polyps (86.3%), sessile and flat lesions (52.2%), GP (55.5%), rectum (64.6%), distal colon (80.2%), proximal colon (60%), T1 carcinomas (25.8%) (p<0.01). En bloc ER was performed in 67.2% of cases, using endoscopic mucosal resection in 8.6% of cases. ER was performed during a single session in 76.8 and at a 2nd procedure by the same endoscopist (18.6%) and by a 2nd expert (5.8%). Surgical resection (SR) was required for 81 polyps (24.9%) (including 49 GP) in 61 patients (21.9%)(mean polyp size 35mm). The main reasons for SR were the failure of ER (44%) and the malignancy (46.7%). 16.3% of SR were transanal, 39.3% laparoscopic and 44.3% open resections. A follow-up colonoscopy was performed in 99 patients (35.6%) after a mean follow-up time of 19.7 months. A recurrence was detected in 26 patients after ER (34.2%), treated by ER, and in 3 patients after SR (17.4%), treated by surgery. CONCLUSION: Our series shows that in the real world one patient with a benign large polyp out of 5 is operated on (2 out of 5 with a benign giant polyp). Referral to surgery is related to the sessile or flat shape of the adenoma, its size, its proximal or rectal location, its malignancy and to the lack of referral to an expert endoscopist. Endoscopic mucosal resection is only performed by a minority of endoscopists and the referral to an expert endoscopist remains rare. AIM To assess the success rate of endoscopic resection of large and giant colorectal polyps in a population-based setting PATIENTS AND METHODS HAUT-RHIN : one of 23 pilot areas for a population-based CRC screening programme 190 000 residents aged 50 to 74 years invited to complete a GFOBT (Guaiac based faecal occult blood test) RETROSPECTIVE STUDY of all large polyps (>2cm) detected over a 3 year period (Sept 2003 to Sept 2006) by 34 endoscopists ( 21 in private practice) in the CRC screening programme CHARACTERISTICS : modality of endoscopic or surgical resection, size and shape of the lesion RESULTS 2968 colonoscopic procedures 325 polyps detected in 279 patients ( 88 polyps in 82 women and 237 polyps in 197 men) 215 large polyps ( size 20 -29 mm) and 110 giant polyps (size > 30mm) POLYPS CHARACTERISTICS ENDOSCOPIC vs SURGICAL RESECTION ENDOSCOPIC RESECTION (N=247 polyps in 218 patients) SURGICAL RESECTION (N=81 polyps in 61 patients) Technical : EMR (endoscopic mucosal resection) (8.6%) en bloc resection (67.2%) Reason for failure : size / location / malignant gross appearance 86% of the large polyps were resected by an expert endoscopist vs 69% by a non-expert endoscopist Technical : transanal n=9 (16.3%) laparoscopy n=37 (39.3%) open resection n=38 (44.3%) Reason for surgery : failure of endoscopic resection (40%) polyposis (9%) malignant polyp (more than 50%) FOLLOW-UP Performed in 99 patients (35.6%) after a mean follow-up time of about 10.2 months Recurrence in 26 patients after endoscopic resection (11.6%) Recurrence in 3 patients treated by surgery (4.9%) CONCLUSION In the real world, 1 patient with a benign large polyp out of 5 is operated on (2 of 5 with a benign giant polyp). Referral to surgery is related to the sessile or flat shape of the adenoma, its size, its proximal or rectal location, its maligancy and to the lack of referral to an expert endoscopist. EMR (endoscopic mucosal resection) is performed by a minority of endoscopists and referral to an expert endoscopist remains too rare (4.6%). Only 50% of giant polyps could be resected endoscopically vs 85% of large polyps (20-29mm). 86% of pedunculated polyps were resected endoscopically vs 50% of sessile or flat lesions. UEGW, PARIS, 2007