Download
1 / 8
90 likes | 208 Views
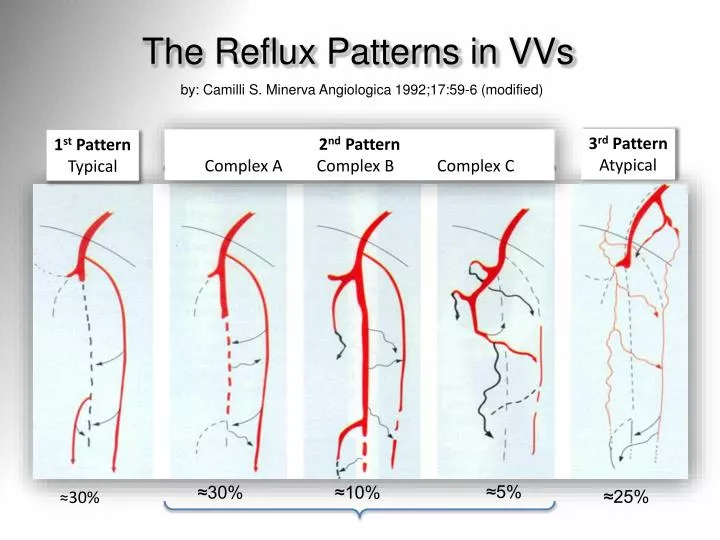
The Reflux Patterns in VVs. by: Camilli S. Minerva Angiologica 1992;17:59-6 (modified). 3 rd Pattern Atypical. 2 nd Pattern Complex A Complex B Complex C. 1 st Pattern Typical. ≈5%. ≈30%. ≈10%. ≈25%. ≈30%. Saphenous nerve injury after EVLA vs. RFA.

E N D
The Reflux Patterns in VVs by: Camilli S. Minerva Angiologica 1992;17:59-6 (modified) 3rd Pattern Atypical 2nd Pattern Complex A Complex B Complex C 1st Pattern Typical ≈5% ≈30% ≈10% ≈25% ≈30%
Saphenous nerve injury after EVLA vs. RFA From: ACP mail (Am Coll Phleb), on Sept 26th 2013 Stephen Konigsberg - Atlanta (GE), USA I have been doing EVLT for 9 years and have occasional saphenous nerve injuries - maybe one or two a year. Recently I have started doing RF ablations and in the past 2 months I have had 6 or more. Does anyone have any insight or experience with SNIs with RFA compared to EVLT? Daniel Mountcastle - Tampa (FL), USA We had a similar experience and sent the machine back ..... enough! Use laser ablation (since 2006 ~7k lasers ). Used RF for too many txs ?20-30 in retrospect. Found too stiff to navigate slight tortuosity. No difference in post op. Thick and must make a nick. One burn using stylet on perf with company rep at my shoulder advising. Alarming clot extension at the SFJ. Dissatisfactory experience. Dropped it.
The matter: Recurrent Varices (ReVa) [1] Carandina S. et Al: Eur J Vasc Endovasc Surg 2008;35(2):230-7 [2] Parès JO et Al: Ann Surg 2010;251(4):624-31
The Matter: VVs Recurrence Diverging lines after 3 yearsf-u [2] Parès JO et Al: Ann Surg 2010;251(4):624-31 [1] Carandina S. et Al: Eur J Vasc Endovasc Surg 2008;35(2):230-7
Recurrence after GSV ablationREVA_TA (thermal ablation) vs. REVA_S (stripping)after 3 yearsmean f-u • SFJ reflux : 43% in REVATA, 47% in REVAS • Neovasc. : 10% in REVATA, 24% in REVAS • Relapsing VVs: 7% out of 2,370 pts • Factors: • Recurrent perforators • GSV recanalisation • Incompetent anterior accessory vein From: VascularNews, 06 Mar 2012 * (presented at iCON 2012) Ronald Bush Palm City (FL), USA * Web: http://www.cxvascular.com/vn-venous-news/vascular-news---venous-news/recurrence-after-ablation-for-varicose-veins-associated-with-perforating-veins#sthash.JpyCYRfR.dpuf
Trials (EVLA, HL+Stripping, SFLigation) Rasmussen L. (DK): J Vasc Surg. 2013;58:421-6 … did not show any significant difference between the two groups Disselhoff BC.(NL). Eur J Vasc Endovasc Surg. 2011;41:685-90 …VVs recurrence was similar in both study groups
GSV Ablation Vs. CHIVA I have a dream… The best option in VVS should be: • Hemodynamic approach, like in CHIVA, by: • DUS + reflux mapping • Valvuloplasty, as a Key Point, to: • repair the valve and stop the reflux • maintain the forward (+ backward) outflow • Conservative GSV strategy by (either): • tributaries disconnection / ablation, by • CHIVA 2nd, Müller, ASVAL, Foam