Download

1 / 17
170 likes | 301 Views
Refining the Black Country Referral Pathways and MDT structure. Regional Progress Presentation October 2012 Helga Becker BCSVN. Refining the Black Country Referral Pathways and MDT structure. The aim:

E N D
Refining the Black Country Referral Pathways and MDT structure Regional Progress Presentation October 2012 Helga Becker BCSVN
Refining the Black Country Referral Pathways and MDT structure • The aim: • To develop a MDT Structure which enables efficient and effective decision making without loss of quality of care during the reconfiguration process • Possible introduction of new working practices and national standards • The necessary referral pathways which support this • Patient needs and benefits at the centre
Refining the Black Country Referral Pathways and MDT structure • The Challenges: • Comment from AAQIP: “SEVERAL units have undertaken this intervention around the U.K but yours is the first across a Network so may be a bit more challenging. “ • Variations in local practice amongst the three Network sites • Need to embed possible changes sensitively, • to a standard of high quality care • “future- proof” • and with full support of all network clinicians • at a generally sensitive time of reconfiguration of services with the practical and emotional challenges this brings to all members of the vascular Multi Disciplinary Team
Refining the Black Country Referral Pathways and MDT structure • TIMELINES: • Outline plan for local implementation of intervention (9th March 2012) • Sent to AAAQIP and Mark Gannon • To include local agreement on team members involved, aims, baseline and ongoing measures of intervention (if available). • Complete survey on QI intervention progress (25th May 2012) • Survey will be sent out from AAAQIP nearer the time to gain feedback on what has happened so far-have any changes occurred in clinical care or patient experience? • West Midland’s AAAQIP Regional Progress Meeting (June 2012). • Feedback given on progress so far • Teams will be selected to produce a 5 minute presentation on their intervention: progress, feedback and learning to date • West Midland’s AAAQIP Regional Progress Meeting (October) 2012).
Refining the Black Country Referral Pathways and MDT structure • Available Documentation: • the AAA pre-operative care bundle, • adaptations from elsewhere, • a care bundle audit form as well as a presentation from Manchester on a similar intervention. • Local Implementation Plan for the network includes a strategy to develop network MDT and referral pathways through the formation of a clinical sub group with membership from all network sites and members of the MDT including specialist nurses and WM ambulance services
Refining the Black Country Referral Pathways and MDT structure • The Process: • Strategy developed in alignment with the existing network implementation plan • Main steps: • Summary of the AAQIP meeting sent to all members of the vascular Multidisciplinary team on all sites in Feb 2012 • Presentation of the project at the Black Country Clinicians’ Meeting held at RHH in February 2012 and the formation of a working group invited as well as comments from Clinicians from all sites on how they would like to see the MDT and Pathways organised • Development of MDT Process and Referral Pathways agenda item for Clinical Subgroup meetings from 19/03/2012 • 1st draft of MDT structure proposal put to discussion at Sub Group Meeting on 24/04/2012 and distributed via email to all members of the clinical subgroup for comment
Refining the Black Country Referral Pathways and MDT structure • The Process: • Strategy developed in alignment with the existing network implementation plan • Main steps, continued: • Referral Pathways- complete • Recruitment of 2 MDT coordinators complete, in post • Network MSH in post since May 2012 • Weekly Network MDT - up and running since June 2012 • Go live date July 2012 successful: phase 1: Vascular Emergencies and AAA repairs • Critical appraisal of functionality of MDT and pathways- ongoing • Learning from mistakes, implementation of necessary improvements by April 2013
Refining the Black Country Referral Pathways and MDT structure AAA screening OP clinics inpatient referrals Draft 1 April 2012 Walsall MDT AAA screening OP clinics inpatient referrals Dudley MDT MDT Model AAA repairs planned ( weekly) Feedback on AAA repairs undertaken (monthly) Signifies feedback through MDT coordinators, minutes and Spoke site representative at Hub MDT AAA screening OP clinics inpatient referrals Wolverhampton MDT Phase 1: AAA’s and emergencies operated at Hub, other elective work done at spoke sites (from 16/07/2012 until April 2013) Local MDT’s continue to be held at spoke sites with feedback to Hub MDT of cases which will be operated at hub MDT Coordinators present at spoke site MDTs Hub MDT open to clincians from all three sites for attendance
Refining the Black Country Referral Pathways and MDT structure AAA screening OP clinics inpatient referrals Current structure 2012 Walsall MDT AAA screening OP clinics inpatient referrals Dudley MDT MDT Model Outcome Feedback through MDT coordinators, minutes and Spoke site representative at Hub MDT Network MDT AAA repairs planned Emergency cases discussed as appropriate prior or post intervention AAA screening OP clinics inpatient referrals Wolverhampton MDT Phase 1: AAA’s and emergencies operated at Hub, other elective work done at spoke sites (from 16/07/2012 until April 2013) Local MDT’s continue to be held at spoke sites Network MDT open to clincians from all three sites for attendance
Refining the Black Country Referral Pathways and MDT structure • "Standards" for MDT Meetings: • Capacity to discuss all vascular patients undergoing investigations/ potentially requiring interventions • Held regularly • Remit/ Terms of Reference • Clerical support • Patient pathway/ journey coordinator • Minimum (quorate) specialist Representation • Technological support • Agenda • Patient database for audit, review, coordination of care and follow up • Minutes • Coordination of discussion outcomes • Lines of communication between different site MDTs Referral pathways "in" • Referral pathways "out" • Clinical Governance Structure
Refining the Black Country Referral Pathways and MDT structure • Problems encountered/ feedback from Members of the MDT • process by which the MDT discussion is recorded in the clinical records at New Cross and at Walsall Record of each individual patient’s MDT discussion now filed in the patient records at New Cross and Walsall • For best assessment of the treatment options for AAAs Ct Image quality at MDT could be improved CT images are generally only presented in their axial format multiplanar reconstruction (MPR) is available in the room but slowand difficult to use in the MDT room ?TeraRecon software • If a clinician’s patient is discussed in their absence there needs to be a robust way of letting them know the outcome of the discussion. Circulation of the MDT minutes on their own may not be sufficient
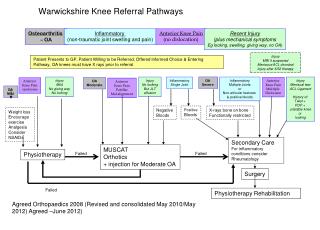
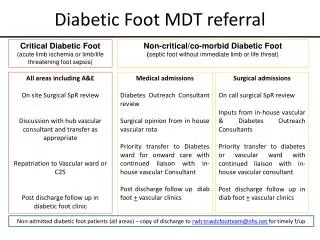
Refining the Black Country Referral Pathways and MDT structure • Referral pathway development: Emergencies • Pathways have been established for: • Leaking AAA – Spoke site, Emergency Department • Acutely Ischaemic leg - Spoke site, Emergency Department • Acutely Ischaemic leg - Spoke site • Diabetic / Ischaemic leg - Spoke site, Emergency Department • Poly Trauma/ Vascular Injuries - Spoke site, Emergency Department • Ilio – femoral DVT - Spoke site, Emergency Department/Ward • Thrombosed / Bleeding AV Fistula - Spoke site, Renal Unit/Emergency Department • Swollen Upper Limb? DVT - Spoke site, Emergency Department • Acutely Ischaemic Arm - Spoke site • Diabetic Foot - Spoke site, Emergency Department/Ward • Critically Ischaemic foot, Black Toe - Spoke site, Emergency Department/OPD/Ward • Post Angioplasty Acutely Ischaemic Leg -/Bleeding , Spoke site
Refining the Black Country Referral Pathways and MDT structure • Referral pathway development: • Elective Procedures • Pathways have been established for: • AAA repairs • Amputations • Carotid Disease • Diabetic Foot
Refining the Black Country Referral Pathways and MDT structure EXAMPLE:AAA
Refining the Black Country Referral Pathways and MDT structure • Where are we now? • Network has gone live in July • MDT and referral pathways are in place • Issues raised surrounding MDT need to be re- discussed and suitable arrangements made – Clinical subgroup task • Need to expand Network MDT for phase 2 (all vascular cases!) for April 2013 • MDT coordinators are in post • Administration of MDT including data collection for clinical governance • Referral pathways have been established
Refining the Black Country Referral Pathways and MDT structure • What’s next? • Work to wards Phase 2 in April 2013 • Finalise MDT arrangements taking into account experiences so far • Revise and adjust Referral Pathways where needed • Scrutinise the implementation and learn from mistakes • Step up patient involvement through satisfaction surveys and follow up
Refining the Black Country Referral Pathways and MDT structure Lots of Room for Discussion! ? Thank you