Download
1 / 29
300 likes | 367 Views
Learn about the musculoskeletal manifestations of Enteropathic Arthropathy related to IBD, such as Peripheral Arthritis and Spondylitis. Discover clinical features, lab tests, radiology findings, treatment options, and differential diagnoses.

E N D
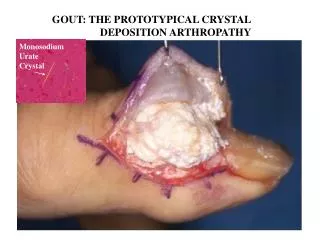
Enteropathic Arthropathy • IBD • INTESTINAL BYPASS ARTHRITIS • WHIPPLE'S DISEASE • Celiac disease
Inflammatory bowel disease • Ulcerative colitis • Crohn’s disease
Inflammatory bowel disease • Intestinal involvement • Extraintestinal involvement
Extraintestinal involvement • Arthritis • Aphthous stomatitis • Erythema nodosum • Anterior uveitis • Pyoderma gangrenosum
Other rheumatic problems • Achilles tendinitis • Clubbing • Hypertrophic osteoarthropathy • Osteoporosis • Vasculitis • Amyloidosis
Musculoskeletal • Peripheral arthritis • Axial arthritis • Both of them
Peripheral Arthritis • Peripheral arthritis : 9 – 30% • More likely in patients with large-bowel disease and in those patients with complications • Male=female • Arthritis may precede symptms of GI especially in children
Peripheral Arthritis • Acute arthritis • Symmetric, migratory polyarthritis affecting primarily large joints of the lower • Associated with a flare-up of the bowel disease • Occurs early • Is self-limiting • Without destruction
Peripheral Arthritis • Lab test: RF – HLA-BW62 Synovial fluids have 5000 to 12,000 white blood cells
Radiology • Soft tissue swelling and effusions without erosions or destruction
Course • Is self-limiting (90% of cases resolve within 6 months) • Responds to successful treatment of the bowel disease
Spondylitis • Frequency : 1.1 to 43% • Spondylitis often precedes IBD • M>F • The activity of spondylitis dose not correlate with activity of IBD
Clinical features • Pain and stiffness in the back and/or buttocks in the morning or after rest • Stiffness and pain are often relieved by exercise • Physical examination reveals limitation of spinal flexion and reduced chest expansion • Some patients may have peripheral arthritis
Lab. test • HLA-B27 : 53 to 75%
Radiology • Typical findings of ankylosing spondylitis and bilateral sacroiliitis
Treatment • Glucocorticoids • Anti-tumor necrosis factor • Sulfasalazine • Colectomy (for ulcerative colitis)
UNDIFFERENTIATEDSpndyloarthropathy • Have some features of one or more of the spondyloarthropathies but there are not enough evidences to meet criteria for differentiated spondyloarthropathies • Are not uncommon • usually young adults
UNDIFFERENTIATEDSpndyloarthropathy • Approximately half the patients with undifferentiated spondyloarthropathy are HLA-B27 positive, and thus the absence of B27 is not useful in establishing or excluding the diagnosis.
Clinical presentations • inflammatory synovitis of one knee, Achilles tendinitis, and dactylitis of one digit ("sausage digit"), or sacroiliitis in the absence of other criteria for AS
Course • Some cases, the patient subsequently develops IBD or psoriasis or the process eventually meets criteria for ankylosing spondylitis.
juvenile-onset spondyloarthropathy • Age : 7-16 • M>f • Asymmetric, predominantly lower extremity oligoarthritis and enthesitis without extraarticular features is the typical mode of presentation
juvenile-onset spondyloarthropathy • SEA syndrome (seronegative, enthesopathy, arthropathy(
juvenile-onset spondyloarthropathy • Prevalence of B27:80% • Many, but not all, of these patients go on to develop typical ankylosing spondylitis in late adolescence or adulthood.