Download
1 / 40
831 likes | 2.61k Views
Charcot Arthropathy. Dr. Saima Hashim Khan Dept. of Diabetes & Endocrinology HMC. PGMI. Case History : 1. 55yrs old married female Type2 diabetic 25yrs HTN 7yrs Swelling right foot >1month, treated as cellulitus with antibiotics. INVESTIGATION. Hb 10.8g/dl, TLC 9900/cmm

E N D
Charcot Arthropathy. Dr. Saima Hashim Khan Dept. of Diabetes & Endocrinology HMC. PGMI
Case History : 1 • 55yrs old married female • Type2 diabetic 25yrs • HTN 7yrs • Swelling right foot >1month, treated as cellulitus with antibiotics
INVESTIGATION Hb 10.8g/dl, TLC 9900/cmm S.creatinine 0.7mg/dl S.uric acid 4.0mg/dl X ray foot.
Case History : 2 • 45yrs old married female • DM2 15yrs (Retinopathy: PRP, Nephropathy: crt clr 103 ) • HTN 5yrs • Post amputation RT big toe 3yrs • Swelling LT foot 2 months, treated as cellulitis with antibiotics
Investigations • Hb:9.5 gm/dl, TLC 9600/cmm • URIC ACID 4.2mg/dl • CREATININE 1.02mg/dl • DOPPLER U/S LT FOOT : no DVT normal arterial flow and subcutaneous edema. • Xray Foot:
Tragic “Rule of 15” • 15% of diabetes Foot ulcer in lifetime of patients • 15% of foot ulcers Osteomyelitis • 15% of foot ulcers Amputation ClinicalCareoftheDiabeticFoot, 2005
Tragic “Rule of 50” • 50% ofamputations • 50% of patients • 50% of patients Transfemoral/transtibial level 2nd amputation in 5 years Die in 5 years ClinicalCareoftheDiabeticFoot, 2005
History of charcot foot Mitchell,1831: The first association between joints and neurological diseases. Charcot 1868: Arthropathy and tabes dorsalis. Jordan 1936: Neuritic manifestation of DM
Charcot’s Foot A Neuropathic Arthropathy Caused by repetitive trauma in the setting of: • Diminished sensation & proprioception • Motor neuropathy results in muscle imbalance & abnormal weight bearing. • “Rocker Bottom Deformity” a convex deformity of the foot’s plantar aspect caused by the collapse of metatarsal bones
Etiology • Peripheral sensory neuropathy is always present +/- motor. • Autonomic neuropathy leads to increased blood flow. • Trauma may be an important precipitating factor, although 2/3rd of patients don’t remember any injury. • Bone metabolism both osteoblastic and osteoclastic activities are increased.
Epidemiology • Incidence : 0.1 – 0.5 % . General: Increased in patients with neuropathy. Diabetics: 3-5% • Common in the 4th or 5th decades of life. • Bilateral in 30 % of patients. • Sex difference : No • Type 1 or type 2: Both are at risk. • Majority: in the mid foot but any bone or joint in the foot or ankle can be affected.
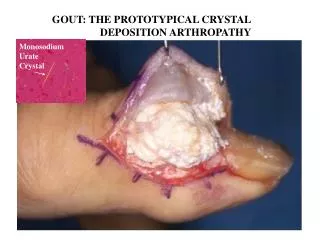
Clinical Features and Diagnosis Acute Charcot • Warm, inflamed and swollen. • Misdiagnosed as cellulitis, osteomyelitis or inflammatory arthropathy as gouty or septic. • Although sensory neuropathy, pain is common feature followed by discomfort. • Diagnosis by exclusion as investigations in early stages are negative.
Clinical Features and Diagnosis High index of suspicion is necessary so that appropriate treatment is immediately instituted to prevent severe deformity!
Clinical Features and Diagnosis Chronic Charcot, may be months, painless, without temperature difference and deformed. • Reactivation by further trauma is frequent. • Patients are at high risk of ulceration and amputation, so long term follow up is recommended.
Investigations • X-ray : Early; absent or subtle finding. Late; bone and joint destruction, fragmentation. • bone scan: Increased bone uptake. • In labeled leucocytes scan to differentiate from osteomyelitis. • MRI: Bone marrow edema is the earliest sign.
Treatment • Immobilization • Pharmacological Treatment. • Surgical Treatment.
Treatment • Immobilization: Almost 16 weeks (3-6 months) but may be more. (temp gradient less than 1 on 2 occasions or serial radiology).
Treatment • Immobilization: • Bed rest • Half-shoes • Crutches, Walkers and Wheelchairs • Total contact cast (TCC) -gold standard • Prefabricated pneumatic walking brace ( Air cast )
Treatment 3. Pharmacological Treatment. • Pilot study first using pamidronate,1994. Other Bisphosphonates were used to decrease disease activity and bone turnover markers. • Calcitonin were also used. • Given for 12 weeks or till temp gradient is less than 2 on 2 consecutive visits.
Treatment • Surgical treatment: No role in acute. Later may be to remove bony deformities or constructive surgeries to achieve a stable shape. Techniques include; Arthrodesis, exostectomies, reconstruction and Achilles tendon lengthening.
Take Home Message • High degree of suspicion to diagnose acute Charcot arthropathy. • High risk categorization. • Immobilization • Bisphosphonate. • Customized Foot Wear