Download

1 / 28
410 likes | 857 Views
The REVERSAL Trial. Reversing Atherosclerosis With Aggressive Lipid Lowering. Atherosclerosis: A Progressive Process. PHASE I: Initiation PHASE II: Progression PHASE III: Complication. Disease progression. Effects of Lipid-Lowering Therapy on CHD Events in Statin Trials.

E N D
The REVERSAL Trial Reversing Atherosclerosis With Aggressive Lipid Lowering
Atherosclerosis: A Progressive Process PHASE I: Initiation PHASE II: Progression PHASE III: Complication Disease progression
Effects of Lipid-Lowering Therapy on CHD Events in Statin Trials Secondary 4S - P 25 prevention Primary 20 prevention 4S - S Simvastatin LIPID - P 15 CARE - P Pravastatin Patients with CHD event (%) HPS - P Lovastatin LIPID - S 10 WOSCOPS - P Atorvastatin CARE - S WOSCOPS - S HPS - S * ASCOT - P S = statin-treated 5 * ASCOT - S P = placebo-treated AFCAPS - P AFCAPS - S *Extrapolated to 5 y 0 90 110 130 150 170 190 210 LDL-C (mg/dL) Modified from Kastelein JJP. Atherosclerosis. 1999;143(suppl 1): S17-S21.
What Is REVERSAL? • Multicenter, randomized, double-blind, active- controlled trial • Comparing the effects of atorvastatin 80 mg/d with pravastatin 40 mg/d administered for 18 months • Using IVUS to measure progression of atherosclerosis
Effects of Lipid Lowering With Statins on Progression of CHD 0.06 Drug Placebo PLAC I 0.05 CCAIT REGRESS 0.04 LCAS PLAC I 0.03 Progression (MLD decrease), mm/y MARS MAAS CCAIT 0.02 MARS REGRESS LCAS 0.01 MAAS 0 -40 -30 -20 -10 0 10 LDL-C reduction (%)
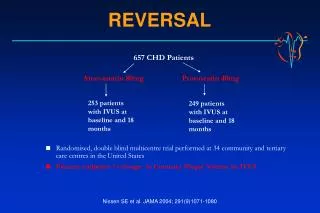
REVERSAL: Study Design Double-blind period Screeningvisit* Placeborun-inphase Atorvastatin 80 mg/d Randomization 654 patients Pravastatin 40 mg/d *Includes baseline IVUS 18-month follow-up with IVUS Design: Prospective, multicenter, randomized, double-blind trial Setting: 34 community and tertiary-care hospitals in the USA
REVERSAL: Study Objective To compare the effects of aggressive lipid-lowering therapy (atorvastatin 80 mg/d) vs moderate lipid-lowering therapy (pravastatin 40 mg/d) on percent change in TAV using IVUS imaging of the coronary arteries in patients with CHD
REVERSAL: Why Was Pravastatin 40 mg Used? • REVERSAL is the first active-controlled, cholesterol- lowering, coronary atherosclerosis progression trial • Previous large-scale trials used placebo as a comparator • Pravastatin has an indication to slow progression of atherosclerosis based on angiographic studies • PLAC I: 264 patients for 3 y vs placebo • REGRESS: 885 patients for 2 y vs placebo • 40 mg was the highest approved dose of pravastatin at the initiation of REVERSAL
REVERSAL: Patient Population • Inclusion criteria: • Patients requiring diagnostic coronary angiography for a clinical indication • Aged 30-75 y • LDL-C 3.2 mmol/L (125 mg/dL) but 5.4 mmol/L (210 mg/dL) • TGs < 6.8 mmol/L (600 mg/dL) • Angiographic inclusion criteria: • Angiographic evidence of CHD defined as 1 lesion with 20% reduction in lumen diameter in any coronary artery • 50% reduction in lumen diameter of the left main coronary artery • The vessel undergoing IVUS evaluation (the “target” vessel) should have 50% stenosis throughout a segment of minimum length 30 mm
REVERSAL: Patient Population • Exclusion criteria: • Target vessel was considered suitable only if the artery had not undergone PTCA or CABG surgery • Left ventricular ejection fraction of < 0.4 • Moderate or more severe CHF • Clinically significant valvular heart disease • Uncontrolled hypertension • Second- or third-degree heart block • Sustained ventricular tachyarrhythmia or an implantedcardiac defibrillator • Known major hematologic, neoplastic, metabolic, gastrointestinal, or endocrine dysfunction
REVERSAL: Primary Efficacy Parameter The percent change from baseline in TAV for all slices of anatomically comparable segments of the target coronary artery as measured by IVUS
REVERSAL: Selected Secondary Efficacy Parameters • Nominal change from baseline in TAV • Change from baseline in PAV • Change from baseline in lipid parameters • Change from baseline in CRP
REVERSAL: Baseline Characteristics Characteristic Atorvastatin 80 mg (n = 253) Pravastatin 40 mg (n = 249) 55.8 ± 9.8 71 90 30.5 ± 6.5 26 20 68 6.0 ± 0.9][231.8 ± 34.2] 3.9 ± 0.7 [150.2 ± 27.9] 2.2 ± 1.2 [197.2 ± 95.7] 1.1 ± 0.3 [42.3 ± 9.9] Age* (y) Male (%) White (%) BMI* (kg/m2) Current smoker (%) Diabetes (%) Hypertension (%) TC* (mmol/L [mg/dL]) LDL-C* (mmol/L [mg/dL]) TG* (mmol/L [mg/dL]) HDL-C* (mmol/L [mg/dL]) 56.6±9.2 73 87 30.5±5.6 27 18 70 6.0 ± 0.9 [232.6 ± 34.1] 3.9 ± 0.7 [150.2 ± 25.9] 2.2 ± 1.1 [197.7 ± 105.6] 1.1 ± 0.3 [42.9 ± 11.4] *Mean ± SD.
Change From Baseline in Lipid Parameters 10 2.9 5.6 0 -6.8 -10 -20 -18.4 Change from baseline (%) -20.0* Pravastatin -25.2 -30 Atorvastatin -34.1* -40 -46.3* -50 TC LDL-C TGs HDL-C *P < 0.001 vs pravastatin. Data are mean percent change from baseline to 18-month follow-up.
P = 0.02 Primary End Point: Percent Change in TAV 3 2.7* 2 Change in TAV (%) 1 0 -0.4† -1 Pravastatin Atorvastatin No significant change frombaseline; atheroscleroticprogression was stopped Significant atheroscleroticprogression from baseline *Progression vs baseline (P = 0.001);†No change vs baseline (P = 0.98).
P < 0.001 Secondary Efficacy Parameters Nominal change in TAV Change in PAV P = 0.02 5 1.8 1.6* 4.4* 1.6* 4 1.5 3 1.2 2 % mm3 0.9 1 0.6 0 0.2† 0.2† 0.3 -1 -0.9† -0.9† -2 0 Atorvastatin Pravastatin Pravastatin Atorvastatin *Progression vs baseline (P = 0.01).†No change vs baseline (P = 0.72). *Progression vs baseline (P < 0.001).†No change vs baseline (P = 0.18).
Change in CRP Levels From Baseline CRP (mg/L) Pravastatin Atorvastatin Baseline 3.0 2.8 18 months 2.9 1.8 0 -5.2 -10 Change (%) -20 -30 -36.4* -40 Pravastatin Atorvastatin *P < 0.001 vs pravastatin.
Nominal Change in TAV for 10-mm Vessel Subsegment With Greatest Disease Severity 0 -1 -1.2* -2 mm3 -3 -4 -4.2† -5 P = 0.01 Atorvastatin Pravastatin *Regression vs baseline (P = 0.049). †Regression vs baseline (P < 0.001).
Selected Prespecified Subgroup Analyses 5 4.8* 4 3.9* 3.2† 3.2* 3 2.5* 2.3† 2.1‡ 2 1 0.7‡ 0.7‡ 0.5‡ 0.2‡ Change in TAV (%) 0 -0.2‡ -1 -0.8‡ -1.2‡ -1.5‡ -2 -2.3‡ -3 -4 Yes No Yes No Median < Median Male Female Diabetes Metabolic syndrome Age Gender *P 0.01 for progression. †P 0.05 for progression. ‡P = NS for progression. Pravastatin Atorvastatin
Percent Change in TAV Among Patients Reaching NCEP ATP III Goal Subgroup reaching NCEP ATP III goal (< 2.59 mmol/L [100 mg/dL]) 161/249 (65%) pravastatin patients (mean LDL-C = 2.27 mmol/L [87.5 mg/dL]) 246/253 (97%) atorvastatin patients (mean LDL-C = 1.75 mmol/L [67.7 mg/dL]) 3 1.9* 2 Change in TAV (%) 1 0 -1 -0.9† Pravastatin Atorvastatin Significant atherosclerotic progression from baseline occurred even among pravastatin patients reaching NCEP ATP III goal *Progression vs baseline (P = 0.01); †No change vs baseline (P = 0.93).
Comparison of LDL-C Reduction and Change in Atheroma Volume Both treatment groups (n = 502) 20 15 10 5 Change in atheroma volume (mm3) 0 -5 -10 -15 -80 -70 -60 -50 -40 -30 -20 -10 0 10 20 % change in LDL-C Regardless of the agent used, an LDL-C reduction of at least 50% was required to halt progression The dashed lines indicate upper and lower 95% CIs for the mean values.Nissen SE, et al. JAMA. 2004;291:1071-1080.
-80 -80 -70 -70 -60 -60 -50 -50 -40 -40 -30 -30 -20 -20 -10 -10 0 0 10 10 20 20 Comparison of LDL-C Reduction and Change in Atheroma Volume Pravastatin group (n = 249) Atorvastatin group (n = 253) 20 15 10 5 Change in atheroma volume (mm3) 0 -5 -15 -20 % change in LDL-C Patients receiving pravastatin who experienced LDL-C reductions > 50% continued to show disease progression The progression rate at any level of LDL-C reduction was lower with atorvastatin than with pravastatin The dashed lines indicate upper and lower 95% CIs for the mean values.Nissen SE, et al. JAMA. 2004;291:1071-1080.
Safety—AEs Atorvastatin 80 mg (n = 327) Pravastatin 40 mg (n = 327) Cardiovascular end point Death (any cause), n (%) 1 (0.3%) 1 (0.3%) MI, n (%) 4 (1.2%) 7 (2.1%) Stroke, n (%) 1 (0.3%) 1 (0.3%) Laboratory abnormality ALT > 3 ULN, n (%) 7/311 (2.3%) 5/316 (1.6%) AST > 3 ULN, n (%) 2/311 (0.6%) 2/316 (0.6%) CPK > 10 ULN, n (%) 0/311 (0%) 0/316 (0%) • Rates of CV end points were similar between groups • Rates of liver- and muscle-enzyme abnormalities were low and similar between groups
Safety—Drug Discontinuations Atorvastatin 80 mg (n = 327) Pravastatin 40 mg (n = 327) Drug discontinuation, n (%) 21 (6.4) 22 (6.7) Musculoskeletal complaint, n (%) 9 (2.8) 12 (3.4) Abdominal complaint, n (%) 3 (0.9) 5 (1.5) Cancer, n (%) 0 2 (0.6) Chest pain, n (%) 0 2 (0.6) ALT/AST < 3 ULN, n (%) 4 (1.2) 0 Other, n (%) 5 (1.5) 1 (0.6)
Summary and Conclusions • First large-scale trial to compare the impact of 2 statins on atherosclerotic disease progression by using IVUS, a more sensitive approach than QCA, to measure plaque burden • There was no change in TAV in the atorvastatin 80-mg group, indicating that atorvastatin stopped the progression of atherosclerosis • Atorvastatin significantly impacted LDL-C, TGs, and the biomarker CRP to a greater extent than did pravastatin • The safety profile of atorvastatin 80 mg was comparable to that of pravastatin 40 mg Treatment with atorvastatin stopped further progression of atherosclerosis
LIPITOR (atorvastatin calcium) is indicated as an adjunct to diet to reduce elevated total cholesterol, LDL-cholesterol, apo B, and TG levels and to increase HDL-cholesterol in patients with primary hypercholesterolemia (heterozygous familial) or combined hyperlipidemia. • In clinical trials, the most common adverse events were constipation, flatulence, dyspepsia and abdominal pain, headache, nausea, myalgia, asthenia, diarrhea, insomnia. • LIPITOR is contraindicated in patients with hypersensitivity to any component of this medication; in patients with active liver disease or unexplained persistent elevation of serum transaminases; myopathy; in women during pregnancy, in nursing mothers, and in women of child-bearing potential not using appropriate contraceptive measures. • Liver function tests should be performed before the initiation of treatment, at 6 and 12 weeks after initiation of therapy or elevation in dose, and periodically thereafter. LIPITOR should be used with caution in patients who consume substantial quantities of alcohol and/or have a history of liver disease. LIPITOR therapy should be discontinued if markedly elevated CPK levels occur or myopathy is diagnosed or suspected.
0 • LIPITOR is available in 10-mg, 20-mg, 40-mg, and 80-mg film-coated tablets, administered once daily. • For further information please see prescribing information. • Lip01FE05 ניאופרם בע"מ בית ניאופרם, רח' השילוח 8, ת.ד. 7063 פתח תקוה 49170, טל-9373737 03, פקס.9373716 03, E-mail:Neopharm@Neopharmisrael.com