Download
1 / 50
500 likes | 511 Views
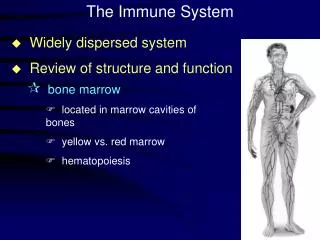
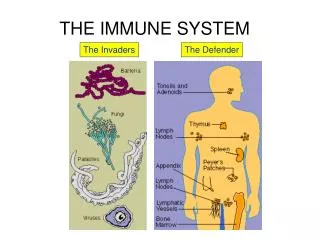
The Immune System. 1: Cells, organs and tissues of the immune system. Cells, organs and tissues of the immune system. The immune system comprises multiple tissues & organs dispersed throughout the body. Lymphoid tissues.

E N D
The Immune System 1: Cells, organs and tissues of the immune system
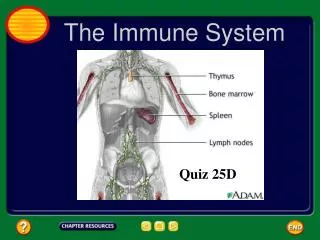
Cells, organs and tissues of the immune system • The immune system comprises multiple tissues & organs dispersed throughout the body.
Lymphoid tissues • These tissues are loosely referred to as lymphoid because they contain a characteristic cell the lymphocyte which also occurs in lymph and is one of the blood leukocytes. • Lymphoid tissues also contain all the other cells described as leukocytes and also non-leukocyte cells described as stromal cells.
Lymphoid tissues • 2 main lymphoid organs & tissues: • PRIMARY - where cells of the immune system develop; • SECONDARY - where the immune response develops. • All lymphoid organs are interconnected by the lymphatic and blood circulatory systems through which cells of the immune system circulate and access non-lymphoid tissues.
Lymphoid tissues • Primary lymphoid tissue includes the bone marrow and thymus; • Secondary includes spleen, lymph nodes and tonsils.
Lymphoid tissues • Leukocytes are not found in significant numbers in other tissues EXCEPT when there is inflammation; • THEN very large numbers of leukocytes will be present, and may form organised collections of cells resembling 2ndry lymphoid tissues.
Cells of the immune system • Leukocytes: • LYMPHOID - lymphocytes of different types • MYELOID - dendritic cells, monocytes/macrophages and granulocytes; • Other cells also involved in immunity: • endothelial cells; • epithelial cells e.g. keratinocytes; • stromal cells of bone marrow • etc.
Cells of the immune system • All leukocytes are generated in primary lymphoid tissue by the process of haematopoiesis. • The lymphoid and myeloid cells follow different differentiation pathways but both are derived from the haematopoietic stem cell, HSC • Go to the website for an outline of haematopoiesis.
Lymphoid cells • These are the cells which are most thought of as characteristic of the vertebrate immune system. • They are antigen specific recognising highly specific characteristics of a pathogenic microbe, generating mechanisms to contain and destroy microbes, and remembering that microbe so that a subsequent encounter generates a more rapid and powerful response.
Lymphoid cells • Antigen specificity and memory are the essence of immunity, and lymphocytes are the essential cells.
Lymphocytes - types • There are two main antigen-responsive types: • B (bone marrow-derived) lymphocytes (B cells); • T (thymus-derived) lymphocytes (T cells). • (A third type is NOT antigen responsive but shares important characteristics • large granular lymphocytes, LGL.)
Lymphocytes - function When activated by cognate antigen: • B cells make antibody & are responsible for humoral immunity; • T cells help B cells and are responsible for cell-mediated immunity (CMI) • antigen-specific killer cells etc; • LGL are natural killer (NK) cells.
Lymphocytes Morphology: • both T & B cells are normally small round cells with little cytoplasm, condensed nuclei, non-dividing & with v. little metabolism: • upon activation develop into lymphoblast (plasma cell if B) - larger, more cytoplasm, dividing. • LGL: larger, with ample, granular cytoplasm.
Normal blood smear showing lymphocyte. Small cell, dark stained (condensed) nucleus, little cytoplasm
NK Lymphocyte morphology transmission EM Lots of cytoplasm with granules hence “large granular lymphocyte” H&E stain. One or 2 regular lymphocytes (?) present (arrows).
infiltrating mononuclear cells tubule Kidney allograft - masses of infiltrating mononuclear cells destroying it
Lymphocytes • These cells are further defined by surface markers: “CD antigens” (also here) • CD stands for “cluster of differentiation” and this originally meant a collection of monoclonal antibodies all recognising a particular protein: by extension, that protein. • Recognised by immunohistochemistry or flow cytometry through used of labelled monoclonal antibodies.
Mature lymphocyte CD (etc) markers Markers specific for: • T cells: two types: all have CD3; TCR; CD25 (last one on activated cells and Treg cells only); and CD4 OR CD8; i.e. “CD4 or CD8 T cells”. • B cells: CD19; CD20; sIg. • LGLs: CD56. (This will do for now.)
T cell subsets • CD4 cells help activation of B and other T cells hence are referred to as helper cells (Th): • there are further subsets of Th cells, Th1 & Th2 (more about these later). • CD8 cells kill other cells which they recognise via TCR and are often referred to as Tc cells or CTL. • Treg cells regulate other T cells • All types produce cytokines.
Cytokines? • These are proteins secreted by a range of cell types that act like hormones • Cytokines are essential for cell-cell communication in the immune system. • More about cytokines later and see: here.
Myeloid cells:antigen non-specific, accessory and effector cells
Myeloid cells • These cells perform essential accessory functions in the activation of lymphocytes; • and are activated either by microbial components or by cytokines or other mediators to become effector cells. • They also produce cytokines. • No memory.
Myeloid cells • Dendritic cells; • Monocytes/macrophages; • Neutrophils/polymorphonuclear leukocytes; • Eosinophils, basophils, mast cells.
Dendritic cells • These are so-called because they have multiple projections (“dendrites”); • They are present in non-lymphoid tissues but never in large numbers • here they pick up antigen and carry it to lymphoid tissues. • Their main role is as accessory cell in the activation of Th cells • particularly on first exposure to a foreign antigen.
Monocyte/macrophages • These are the same cell but in different differentiation states: monocytes are present in the circulation but become macrophages when they migrate into the tissues. • Macrophages are so-called because they are large & phagocytic.
Normal blood smear (same as 16) showing monocyte and lymphocyte. The monocyte is the bigger cell, dark stained, some cytoplasm.
Monocyte/macrophages When activated: • Macrophages can function as an accessory cell in T cell activation; • and are potent anti-bacterial cells through their phagocytosis. • macrophages in lymph node here (lower frame); • sooty macrophages in lung here.
Neutrophils/polymorphonuclear leukocytes • These are so-called because they stain with neutral stains, and have odd nuclei, somewhat granular cytoplasm. • Their principal role is in resistance to bacteria which they phagocytose and kill as do macrophages.
Normal blood smear (same as 16) showing 2 neutrophils. Big cells, bizarre nucleus, much cytoplasm.
Eosinophils • These are so-called because they stain pink with eosin in standard histological stains. • Their principal role is in resistance to parasites BUT they also mediate allergy.
Normal blood smear (same as 16) showing eosinophil (top right). Big cells, much cytoplasm with abundant pink (eosinophilic) granules. Compare neutrophil bottom left)
Basophils & Mast cells • Basophils are so-called because they stain dark with basic stains in standard histological stains. • They and their close relatives mast cells (found in tissues) function much as eosinophils.
Leukocytes • Fuller descriptions and pix of all these cells can be found in any text book or at http://www.wadsworth.org/chemheme/heme/microscope/celllist.htm
Organs and tissues: schematic anatomy in the context of the immune response
Organs & tissues … • I am not an anatomist & cannot deal in any detail with the gross or microscopic anatomy of the immune system … • Instead I will describe how the immune system is organised in order to facilitate the response to an invading microbe. • Use Kumar etc. to mug up on detail, particularly how the 2ndry tissues work.
Organs & tissues … • A key point in immunity is that antigen specific cells are rare upon FIRST encounter (why this is will be dealt with later) and the structure of the immune system is adapted to maximise the chances of an antigen meeting its cognate lymphocyte.
Organs & tissues … • Most infections start locally but may disseminate. • Dissemination is via the circulation • lymphatic; • blood. • The immune response mirrors this.
Organs & tissues … • At the initial site of infection, inflammation will occur • more about this later. • Inflammation is extremely important in directing leukocytes to the site of infection.
Organs & tissues … • The adaptive immune response gets under way when antigen encounters lymphocytes bearing cognate receptors. • This occurs in the local lymph node. • Antigen will be transferred either free or (more important) by dendritic cells to the local lymph node via lymphatic drainage.
Organs & tissues … • The role of the lymphatic system is to drain fluid from the tissues via lymph nodes to the blood system. • Pathogens in the tissues will be transported to the lymph node, where the adaptive immune response develops.
Organs & tissues … • The lymph node is a bag of cells many of which are lymphocytes. • The structure & cellular make-up of the tissue is adapted to maximise the interaction between lymphocytes and antigen and so maximise the chance of the rare antigen specific cell meeting its cognate antigen.
afferent lymphatics (to) Structure of a lymph node high endothelial venules capsule vein efferent lymphatic (from) artery
Section of the cortex of a lymph node Germinal centre aka secondary follicle: activated B lymphocytes surrounded by mantle zone of resting B lymphocytes. primary follicle: resting B lymphocytes paracortex: mostly T lymphocytes red = B cells blue = T cells
Organs & tissues … • The probability of receptor-bearing cell meeting cognate antigen is further increased by the circulation of lymphocytes, which exchange between blood & lymphatic circulation & tissues.
bm = basement membrane Schematic of leukocyte circulation
Organs & tissues … • The effector mechanisms then develop in the lymph node. • The final step is to transfer the immune effectors from the lymph node to the site of infection. • This is via the blood circulation. • Cellular effectors localise at the site of the infection because of the inflammation there.