Download
1 / 68
730 likes | 1.65k Views
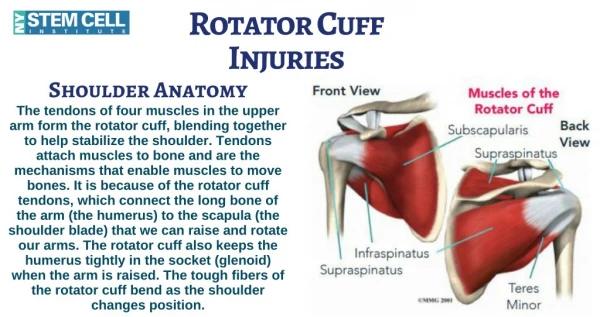
Rotator Cuff Tears. Daniel Penello Upper Extremity Rounds 22 Feb 2006. Anatomy. Subscapularis. Long Head of Biceps. Function. “Fine-tuning” muscles Keep the humeral head centered on the glenoid regardless of the arm’s position in space.

E N D
Rotator Cuff Tears Daniel Penello Upper Extremity Rounds 22 Feb 2006
Anatomy Subscapularis Long Head of Biceps
Function • “Fine-tuning” muscles • Keep the humeral head centered on the glenoid regardless of the arm’s position in space. • Generally work to depress the humeral head while powerful deltoid contracts
Pathophysiology • Intrinsic Factors • Vascular supply (? significance) • Distal 1cm of supraspinatus tendon (early studies) • Hypervascularity with tendonitis • Degenerative changes • Age related • Change in proteoglycan and collagen content in symptomatic tendons
Pathophysiology • Extrinsic factors • Impingement • Acromial spurs • Type III acromion and decreased geometric area of the supraspinatus outlet • Increased prevalance of symptomatic cuff disease • Coracoacromial ligament • AC joint osteophytes • Coracoid process • Posterior superior glenoid
Pathophysiology • Extrinsic factors • Repetitive use • Tensile overload • Muscle fatigue • Microtrauma • Glenohumeral instability • Accentuates abnormal loading • Can lead to internal impingement
Incidence • Lehman - Bull Hosp Jt Dis 1995 • 235 cadavers • overall incidence full thickness tears 17% • < 60 yo = 6% • > 60 yo = 30% • Yamanaka & Fukuda 1983 • partial thickness tears 13% incidence • commonly intratendinous • < 40 yo = 0% • > 40 yo = 30%
Incidence • Sher et al. JBJS-A 1995 • MRI asymptomatic volunteers • Normal, painless function • 19 to 39 • 0% full thickness • 4% partial (1 of 96) • 40 to 60 • 4% full thickness • 24% partial thickness • Over 60 years old --> 54% incidence • 28% full thickness • 26% partial thickness
Classification Partial Bursal vs Articular < 50% thickness > 50% thickness Complete Organize by size Number of muscles involved
Mechanism Traumatic vs Chronic/Insiduous
As larger muscles fatigue, the posterior capsule and rotator cuff play a larger role in decelerating the arm. Leads to tensile overload and fatigue Pitching
Pitching • As rotator cuff fatigues, it no longer performs it’s role in keeping the humeral head centered. • This leads to superior migration of the humeral head and impingement. • This leads to pain and muscle inhibition…. • ……and the cycles repeats itself
Pain and/or fatigue of cuff Rotator Cuff dysfunction Impingement with motion
Posterior Capsular Tightness • As a result of microtrauma and inflammation. • Capsule tightens and can no longer accommodate humeral head as it rotates. • Leads to obligatory anterior-superior migration of humeral head. • Reduces subacromial space
History • Pain on the lateral aspect of the shoulder • may radiate to deltoid insertion • anterior acromion with impingement • +/- biceps tendonitis • Stiffness, esp IR • Cannot lie on that side • Weakness, instability, crepitus • Partial tears more sore and stiffer • Acute tear may have inciting event
Physical Exam • Inspection: atrophy, symmetry • Palpation: AC, cuff tenderness • Range of motion: active, passive • Strength: ER and elevation power, lag • Provocative: impingement sign, arc of pain
Physical Exam • Impingement testing NEER SIGN • Shoulder internally rotated, examiner forward flexes the patient’s arm, pushing the supraspinatus against the anteroinferior acromion, with increased shoulder pain signifying rotator cuff inflammation or tear
Physical Exam • Impingement testing Hawkin's test • With patient’s arm abducted to 90°, then shoulder internally rotated, pushing the supraspinatus against the anteroinferior acromion, with increased shoulder pain
Physical Exam • SUBSCAPLULARIS • Gerber's lift off test: push examiner's hand away from 'hand behind back position' • Internal rotation lag sign: inability to hold hand away from back • Napoleon test: if pt cannot fully internally rotate, pt. pushes on their belly, elbow will drop backwards if +ve
Physical Exam SUPRASPINATUS • Jobe's Test: arm abducted in the plane of the scapula, thumb pointing down . Resist elevation of the arm.
Physical Exam • INFRASPINATUS • Resisted ER with arm by side activates both infra and Teres minor equally, therefore not specific. • Place arm by side, flex elbow 90 degrees, ER 45 degrees and resist internal rotation of arm. Mostly infraspinatus
Physical Exam • TERES MINOR Hornblower's sign: 90º shoulder abduction, elbow 90º, resisted ER (teres minor)
Physical Exam • Long head of biceps testing • Speed’s test • FF 90, elbow 0, supinated forearm • resisted downward force • biceps or SLAP • Yergason’s test • With patient’s arm at side with elbow flexed 90° and forearm pronated, examiner resists supination of the forearm --> pain or tendon subluxation out of groove
Physical Exam • Deltoid • resisted abduction at 90 • Serratus anterior • winging
Physical Exam • AC joint testing Horizontal adduction • forced cross body adduction in 90ºflexion, pain at the extreme of motion indicative of ACJ pathology
Imaging • Plain radiographs • AP • glenohumeral arthritis, calcific tendonitis, migration of humeral head superiorly, greater tuberosity changes (cysts or sclerosis indicating chronic tear) • Transcapular lat
Imaging • Plain radiographs • Axillary • subluxation, os acromiale (association with rotator cuff tears - beware excision with acromioplasty) • Supraspinatus outlet • 10 to 15 degree caudal tilt of transcapular lateral • can see acromial spurs well • AC joint • 10 to 30 degree cephalad tilt of AP
Ultrasound • Teefey JBJS-A 2000 - Ultrasonography of the Rotator Cuff. A Comparison of Ultrasonographic and Arthroscopic Findings in One Hundred Consecutive Cases • CONCLUSIONS: Highly accurate for full thickness tears Poor accuracy for partial thickness tears
Full thickness Partial thickness
Ultrasound • Technician dependent • Can be a dynamic study • Easier to obtain • Hard to read
MRI vs Ultrasound • Detection and quantification of rotator cuff tears. Teefey et al. JBJS 2004 • 71 patients with shoulder pain had imaging with U/S and MRI then underwent arthroscopy • 46 full thickness tears • 19 partial thickness tears • 6 had no tear • U/S and MRI had comparable accuracy for identifying and measuring size of partial and full thickness tears • MRI slightly more sensitive
MRI • Static study • More expensive • Longer wait-list • Can assess intra-articular pathology, such a labral tears. • Easier to read
Differential Diagnosis • Rotator Cuff Tendinitis • Partial Thickness Rotator Cuff Tear • Calcific Tendinitis • Acromioclavicular Joint Pain • Adhesive Capsulitis • Glenohumeral Joint Arthritis • Thoracic outlet syndrome • Suprascapular Nerve Entrapment or brachial neuritis (rarely)
Natural History • Yamanaka & Matsumoto - CORR 1994 • 40 pts with partial thickness tears • avg age 61, conservative Rx • @ 1 year • 21 pts tear increased in size • 11 pts full thickness • OVERALL SHOULDER SCORES BETTER
Treatment • Mainstay is conservative • Surgery reserved for significantly symptomatic patients who have failed conservative management > 6 -12 months • Younger patient (<60) with acute tear • Cuff repair within 6 weeks
Non-Operative Treatment • 33-90% successful (Campbell’s) • Candidates: • Partial thickness tears • Older patients with chronic large tears and extensive cuff muscle atrophy • NSAIDs • Symptom control ±↓ inflammation
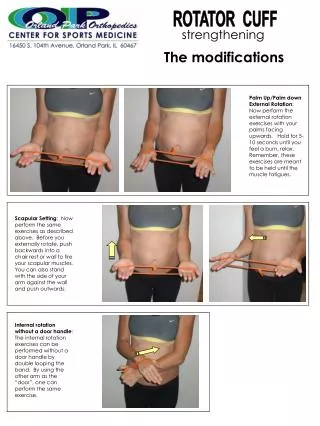
Non-Operative Treatment • Therapy - Stretch posterior capsule with Sleeper Stretch WRONG
Non-Operative Treatment Therapy • Regain full, pain-free ROM • Strengthen all rotator cuff muscles - Isometrics first - Isotonics with theraband • Strengthen shoulder girdle muscles • Improve biomechanics and proprioception
Subacromial Cortisone Injection vs Lidocaine • Corticosteroid injections • Blair & Zuckerman JBJS-A 1996 • Subacromial impingement RCT • Subacromial corticosteroid vs lidocaine
Cortisone vs Lidocaine Pain • At ~30 week F/U • Significant differences in pain, negative impingement sign, active forward elevation & external rotation • Insignificant differences in internal rotation, performance of activities of daily living
Indications for Surgery • Failed conservative management • 3 to 12 month course of NSAIDs, physio, corticosteroid injections, activity modification • Significant or progressive weakness, esp. acute • Early repair if <50 y.o. and full-thickness tear • Differential diagnosis confirms weakness is from rotator cuff tear (i.e. MRI findings correlate with exam, rule out other causes)
Contraindications to Surgery • Asymptomatic tear • Chronic “massive” irreparable tears • Tendon retraction past glenoid rim • Fatty degeneration of muscle • Increased width of subtrapezial fat pad • Frozen shoulder • Need ROM pre-op • Unwilling or unable to participate in post-op physio
Surgical Principles • Neer JBJS-A 1972 • Repair Deltoid to Bone • adequate subacromial decompression • mobilization of muscle-tendon units • secure fixation of tendon to GT • closely supervised rehab