Download
1 / 59
610 likes | 697 Views
Learn about the definition, stages, and management of labor and delivery. Explore essential factors, true vs. false labor, and the clinical course of childbirth.

E N D
Objectives • Definition of labor • True labor • Essential factors of labor • Stages of labor • Clinical course and management of stages
Definition (1) Labor and delivery are the culmination of approximately 280days of preparation. Labor is the process by which the viable products ofconception (fetus, placenta, cord and membrane ) are expelled from the uterus. (whole process, series of events ,viable fetus) It is defined as the progress effacement and dilation of the cervix, resulting from rhythmic contraction of the uterine musculature. preterm labor—prior to 37 completed weeks
Definition (2) The term delivery refers only to the actual birth of the infant at the end of the second stage of labor. it is the expulsion or extraction of a viable fetus out of the womb. it is not synonymous with labor,delivery can take place without labor as in elective C.S. Delivery may be vaginal either spontaneous or aided or it may be abdominal.
Definition (3) • Normal labor (eutocia) : labor is called normal if it fulfils the following criteria. 1) spontaneous in onset and at term. 2) with vertex presentation. 3) without undue prolongation. 4) natural termination with minimal aids. 5) without having any complications affecting the health of the mother and /or the baby.
Definition (4) • Abnormal labor (dystocia): any deviation from the definition of normal labor. • Date of onset of labor:it is very much unpredictable to foretell precisely the exact dete of onset of labor.it not only varies from case to case but even in different pregnancies of the same individual.
Ture labor or in labor • Painful uterine contractions • Increasingly intense and frequent • Is associated with progressive cervical effacement and dilation • Regular contraction occur every 5 minutes, duration lasts more than 30 seconds
False labor and true labor 1.discomfort is characterized as over the lower abdomen and groin areas 2.without effect on dilation of the cervix (not associated with progressive dilation ) 3.typically shorter in duration 4.less intense 5.relieved by administration of a sedative or ambulation 1.over the uterine fundus,with radiation of discomfort to the low back and low abdomen. 2. Associated with effacement and dilation 3. Increasingly intense and frequent 4. Regular and effective
Essential factors of laborLABOR FORCE uterine contraction include three parts: intensity duration frequency
Essential factors of laborLABOR FORCE • Intensity of contraction: it describes the degree of uterine systole. The intensity gradually increases with advancement of labor until it becomes maximum in the second stage during delivery of the baby. During the first stage intrauterine cavity pressure is raised to 40-50mmHg and during second stage it is raised about to 100-120 mmHg. Frequency: in the early stage of labor, the contraction come at intervals of 10-15 min. The intervals gradually shorten with advancement of labor until in the second stage, when it comes every one or two minutes.
Essential factors of laborLABOR FORCE Duration: in the first stage, the contraction lasts for about 30-40 seconds initially but gradually increases in duration with the progress of labor. Thus in the second stage, the contractions last longer than in the first stage.
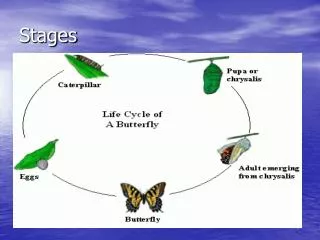
Stages of labor (1) Although labor is a continuous process, it is divided into three functional stages: first stage ------ dilation of cervix second stage ----- fetus delivery third stage -------- placenta delivery fourth stage ------- within 2h after delivery
Stages of labor(2) • First stage: it starts from the onset of true labor pain and ends with full dilation of the cervix. 8-12 hr The first stage is further divided into two phases, the latent phase and the active phase. In the latent phase, cervical dilation is under 3 cm, the contractions may be infrequent, are usually not more than moderately strong and the patient can tolerate, in active phase, more rapid cervical dilation occurs,usually beginning at approximately 3cm .
Stages of labor(3) Second stage: (giving birth): it starts from the full dilation of cervix and ends with expulsion of the fetus from the birth canal. Its duration is 1-2 h in primigravidae, 30 minutes in multiparae. Third stage: it begins immediately after delivery of the infant and ends with the delivery of the placenta. Its average duration is about 15 minutes in both primigravidae and multiparae.
Stages of labor(4) • Four stage: (after deliver of baby and placenta, observing uterus and bleeding) it is defined as the immediate postpartum period of approximately 2 hr after delivery of the placenta. During this time the patient’s general condition and the behavior of the uterus are to be carefully watched. The maidwife monitors the amount of blood as well as pulse and blood pressure in the first several hours after delivery to identify excessive blood loss.
In the first stage 1. Events of the first stage (1) Cervical effacement and dilation Effacement of the cervix is a process of thinning out which is accomplished during first stage of labor or even before that in primigravidae. Taking up is effected by retraction. Expulsion of mucus and the compression effect also help in thinning of the cervix.
In the first stage 1. Events of the first stage The degree of cervical effacement is expressed as percent effacement. i.e. A cervix that is thinned to one-half of its original 2cm length is termed 50%,whereas a cervix that is virtually totally thinned is described as 100% effaced. The dilation of cervix is described as centimeters of dilation. Fig .
In the first stage 1. Events of the first stage • (2) formation of uterine segment
In the first stage 2.Clinical features (1) (1) Pain---- come from the intermittent uterine contraction initially, the pain are not strong enough to cause discomfort and come at varying intervals of 15-30 min with duration of about 30 seconds. But gradually the interval becomes shortened with increasing intensity and duration so that in late first stage the contraction comes at intervals of 2-3min and last for about 50-60 seconds.
In the first stage 2.Clinical features (2) • Fear --- although the patient may have undergone some education regarding the labor and delivery process, it is important to realize that the patient has significant fear that remain. A support person may be allowed to remain with the patient throughout the labor and delivery process in most cases. At no time in labor should the women be left alone. The partner should be with all the time, and midwife as much as possible.
In the first stage 2.Clinical features (3) • (3) Micturation--- during the course of labor, descent of the fetus causes the bladder to be elevated relative to the lower uterine segment and cervix. this often results in the patient having difficulty voiding. The patient, therefore, be encouraged to void frequently. Catheterization may become necessary if the bladder becomes distended
In the first stage 2.Clinical features (4) (4) Diet --- during labor there is delay in the emptying time of the stomach and food or fluids may remain there for several hours. Solid food should be avoid intake. The diet should be liquid with sufficient food value and pleasant to take.
In the first stage 2.Clinical features (5) • Dilation and taking up of the cervix --- by vaginal and rectum examination the dilation and taking up is found. Cervical dilation is expressed in terms of centimeters. It is usually measured with fingers but recorded in centimeters. One finger equals to 1.6 cm and when the dilation is more than 6 cm, it is easier to subtract twice the width of the remaining ‘rim’ from 10 cm to measure the actual dilation.
In the first stage 2. Management (1) 1) admitted to hospital reasons: a. if their contractions occur approximately every 5~10 min for at least 1 hr b. If there is a sudden gush of fluid or a constant leakage of fluid c. if there is any significant bleeding d. If there is significant decrease in fetal movement
In the first stage 2. Management (2) 2) evaluation for labor a. taking history in detail and review perinatal records (LMP, EDC,vaginal bleeding, infectious disease,...) b. A limited general physical examination is performed. Pay special attention to vital signs.
In the first stage 2. Management (3) c.Abdominal examination: The initial examination of the gravid abdomen may be accomplished using Leopold maneuvers, a series of four palpations of the fetus through the abdominal wall that helps accurately determine fetal lie, fetal presentation, and fetal position. The fetal heart rate is checked and any abnormality of rate or rhythm is noted.
In the first stage 2. Management (4) d. Vaginal examination: (dilation and station) • the vaginal examination should be performed using an aseptic technique, in the presence of significant bleeding , the vaginal examination should be done with extreme care. Before any digital examination a sterile speculum examination should be performed. The digital portion of the vaginal examination allows the examiner to determine the degree of cervical effacement. The cervix is also palpated for cervical dilation described as centimeters of dilation. The examiner uses one or two fingers to identify the diameter of the opening of the cervix.
In the first stage 2. Management (5) The following information are to be noted and recorded carefully when performing vaginal examination: ( 1) degree of cervical dilation in centimeters ( 2) degree of effacement of cervix ( 3)status of membranes and if ruptured-color of the liquor ( 4) presenting part and its position by noting the fontanelles and sagittal suture in relation to the quadrants of the pelvis ( 5) station of the head in relation to ischial spines
In the first stage 2. Management (6) 4) Fetal monitoring The fetal heart rate is counted with a stethoscope at half hourly intervals in early labor and at 10 min intervals in the active phase of labor. The normal rate 120 ~ 160 beats per minute and there is no change of rate, or only a very transient showing, with the uterine contractions. Most hospital have employed fetal monitoring during labor, the uterine contractions can be recorded .
In the first stage 2. Management (7) 5) relief of pain Towards the end of the first stage the pains become more severe. The epidural analgesia should be employed. If it is not employed, drugs such as pethidine 100mg intramuscularly may be given if the woman is distressed
In the second stageEvents of the second stage • This stage is concerned with the descent and delivery of the fetus through the birth canal.
In the second stage clinical features • painful contraction is stronger and more frequent; • bearing birth efforts:the expulsive force of uterine contraction is added by voluntary contraction of the abdominal muscles called “bearing down” efforts. In majority, the pushing down efforts start just prior to full dilation of the cervix. It is of immense help in accelerating the expulsion of the fetus. At the height of uterine contraction, the woman closes her glottis, holds her respiration at the height of inspiration,clutches whatever is available and voluntarily contracts the abdominal muscles in an attempt to expel the fetus out of her womb. The face becomes flushed, the neck veins are prominent, the pulse rate is rapid and there is perspiration.
In the second stage clinical features • descent of fetal head---features of descent of the fetus are evident from abdominal and vaginal examination. • Vaginal signs:as the head descends down, it distends the perineum, the vulval opening looks like a slit through which the scalp hairs are visible. During each contraction, the perineum is markedly distended with the overlying skin tense and glistening and the vulval opening becomes circular.
In the second stage clinical features • Vaginal signs: the adjoining anal sphincter is stretched and stool comes out during contraction. The head recedes after the contraction passes off but is held up a little in advance because of retraction. Ultimately, the maximum diameter of the head stretches the vulval outlet and there is no recession even after the contraction passes off. This is called the crowning of the head.
In the second stage clinical features • The perineum, including the anal sphincter, is very much stretched and the anterior rectal wall is visible. The head is born by extension. After a little pause, the mother experiences further pain and bearing down efforts to expel the shoulders and the trunk.
In the second stage clinical features • Maternal signs: there are features of exhaustion. Respiration is slowed down with increased perspiration. During the bearing down efforts, the face becomes congested with neck veins prominent. Immediately following the expulsion of the fetus, the mother heaves a sigh of relief. • Fetal signs: bradycardia during contractions is very much prominent which often continues because of quick successive contractions.
In the second stage management • Principles: To assist in the natural expulsion of the fetus slowly and steadily To prevent perineal injuries • Preparation for delivery ( dorsal position, catheterise the bladder) • Conduction of delivery:delivery of the head, delivery of the shoulders, delivery of the trunk
Once the head is crowned the woman should be discouraged from bearing down by telling her to take rapid shallow breaths. The head may now be delivered carefully by pressure through the perineum onto the fore part of the head by means of a finger and thumb placed on either side of the anus, pushing the head forwards slowly before it is allowed to extend and complete its delivery and controlling the rate of escape with the other hand. The left hand is preventing sudden expulsion of the head, while the fingers and thumb of the right hand are gently helping the head forwards by pressure on each side of the anus.
In the second stage management Delivery of the head--- to maintain flexion of the head, to prevent its early extension and to regulate its slow escape out of the vulval outlet.
In the second stage management • delivery of the shoulders,
In the second stage management • Delivery of the trunk: after the delivery of the shoulders, the fore finger of each hand are inserted under the axillae and the trunk is delivered gently by lateral flexion.
The mouth and pharynx are sucked clear with a mucus extractor, a healthy baby breathes and cries very soon after it is born, if it fails to do so the baby needs active resuscitation. Normally the cord should not be clamped until the child has cried vigorously and pulsation in the cord has ceased. So in the second stage the principle is (1) to assist in the natural expulsion of the fetus slowly and steadily,(2) to prevent perineal injuries.
In the third stage • The third stage of labor comprises the phase of placental separation, its descent to the lower segment and finally its expulsion with the membranes Placental separation : At the beginning of labor, the placental attachment roughly correspond to an area of 20 cm in diameter. During the second stage, there is slight butprogressive diminution of the area following successive retractions, which attains its peak immediately following the birth of the baby.