Download
1 / 75
750 likes | 771 Views
Plagued by parasites! Flies, fleas and dreadful disease. A journey into the delightful world of ectoparasites and the diseases they transmit. Philippe Lagacé -Wiens, MD, FRCPC, DTM&H. Objectives. Be able to tell dinner party guests what an ectoparasite is.

E N D
Plagued by parasites! Flies, fleas and dreadful disease. A journey into the delightful world of ectoparasites and the diseases they transmit. Philippe Lagacé-Wiens, MD, FRCPC, DTM&H
Objectives • Be able to tell dinner party guests what an ectoparasite is. • Name four ectoparasites that commonly irritate travellers and explain how they present clinically. • Name three diseases transmitted by ectoparasites. • Describe the three main types pf plague and explain how ectoparasites play a role in the transmission of plague in Madagascar and elsewhere.
Outline • Introduction to ectoparasites • Common ectoparasites encountered by travellersand the diseases they transmit. • Ticks • Mites and chiggers • Fleas • Botflies • Lice • Haematophagous bugs
Question #1 • The WRHA policy required me to wear this outfit because the patient I was about to see had been exposed to: • Plague • Fleas • Bedbugs • TB • Ebola
Question #2 • What is the difference between a blood sucking arthropod, an vector and an ectoparasite?
What is an ectoparasite? • Parasite- Refers to an organism that benefits from another in a detrimental way, and who is dependent on it’s host to complete it’s life cycle. • Ecto parasites are parasites that live on or in close proximity to, or persistently stays on it’s host. • Most, but not all, ectoparasites are arthropods. • May be persistent (scabies) or transient (ticks). • Generally excludes arthropods that are transient feeders, can survive without a host and generally away or far from the host. • Some are vectors for serious diseases (like PLAGUE!)
A web of bad stuff Kind of gross and annoying: Scabies, (most) mites, myiasis flies. Small group. Mostly made up of teenaged children. Kind of gross and annoying too. Bedbugs, human flea, head and pubic lice. Worst of all worlds: Ticks, kissing bugs, body lice, rat flea… Generally just annoying. Most midges, most biting flies. Small group. Mostly made up of preschool children. Annoying and scary: Mosquitoes, sandflies a few midges, tsetse flies, a few black flies and deer flies.
Basic introduction • Ectoparasites are organisms that live on, in very close proximity or partially intradermally consuming host resources, for the purpose of reproduction, while providing no benefit to the host. • Some are virtually harmless, some a transient annoyance, some are chronically annoying. • VERY few are life threatening, but many transmit diseases that are potentially life threatening.
Epidemiology • No good data exists on epidemiology of ectoparasitic infections. • 10-15% of skin problems in travellers presenting for care are arthropod-related. • Prevalence of bedbugs is greatly increasing globally. • Global population has increased by 100-500% per year! • Global increase in travel and tourism will increase the interface with ectoparasites. • Role of climate change? • Outbreaks and cases of ectoparasite-borne diseases are increasing. J Trav Med. (2006) 13:100-111 International Journal of Infectious Diseases (2008) 12, 593—602 Arch Dermatol Res. 2016; 308(8): 531–538.
Recent ectoparasite-associated outbreaks and emerging diseases • Plague in Madagascar (2017-now) • >2000 cases with >400 deaths. • Several other countries at risk • Lyme borreliosis and anaplasma in Manitoba. • Scabies in USA (2017) • Tick-borne encephalitis in Switzerland (2017) • Scrub typhus in Thailand, Nepal, Cambodia (2015-present). • Borreliamiyamotoi, Borreliamayoniiand Powassan virus in NE USA and Canada (2016-17). • Bartonellosis in USA (2016) www.promed.com
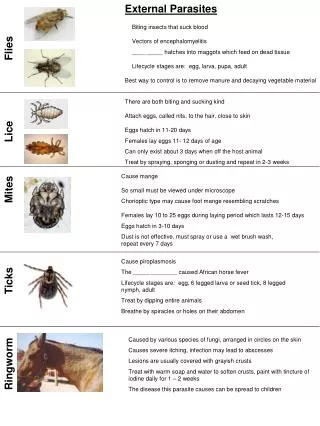
Ectoparasites encountered by travellers • Mites: Scabies and chiggers. • Fleas: Human, cat, dog, rat and chigoe. • Ticks: More types than can be mentioned. • Flies: Myiasis – many kinds • Lice: Head, body and pubic. • Haematophagus bugs: Triatomines and bedbugs
Mites • Mite infestations are extremely common among travellers. • Most tropical destination travellers will experience some form of mite infestation. • Occurs in all common destinations, including popular Caribbean and Mexican resorts. • Most common infestation is by harvest mites (commonly called chiggers). • Scabies can be acquired by travellers.
Chiggers/harvestmites • Over 700 species exist. - Almost all are nuisance ectoparasites. • Larvae burrow into skin and secrete lytic and immunogenic enzymes leading to local irritation. • A delay of 3-7 days before symptoms occur is typical. • Usually drop off before irritation begins. • One species in South and Southeast Asia (Leptotrombidium akamushi) transmits Orientia tsutsugamushi – Scrub typhus • Prevention is by covering exposed skin near the ground/grass.
Harvest mites • Lesions are typically on exposed skin on lower extremities. • Any exposed skin kept low-to the-ground. • History usually includes walking in grassy areas. • May be single to multiple, papule to hive, typically pruritic. • May continue to appear after exposure ends. • Prevention is by covering exposed skin near the ground/grass. • Management is symptomatic with reassurance.
Scabiesmites • Mites reside in the superficial skin, consuming keratinized skin and producing excrement and eggs. • Itch results from reaction to excrement. • Transmissible from person-to-person. • Travellers with close contact with local populations where infestation rates are high are at highest risk.
Scabies • Causes rash, severe itching and often visible burrows in affected skin. • Usually papules or small pustules. Vesicles less common. Nodules may be seen in axillae, groin, penis, scrotum. • Itching caused by hypersensitivity to mite excrements and secretions • Primary scabies has a long incubation time (~3-6 weeks). Subsequent infections present within days of exposure. www.UpToDate.com Topics: Scabies
Body distribution • Commonly affected areas: • Webs of the fingers • Flexor aspects of the wrists • Extensor aspects of the elbows and knees. • Axillary folds • Periumbilical areas • Buttocks and thighs • Scrotum and penis may be affected in men. • Periareolar area in women. www.UpToDate.com Topics: Sabies
Management • Topical agents (5% permethrin) are the mainstay of therapy. • Apply from jawline to toes. Reapply in one week. Duration of treatment varies by product, usually 8 – 12 hours. • Children should have scalp and head treated. • Household and close contacts must be treated simultaneously. • Ivermectin in 2 doses 2 weeks apart is equally effective. • Symptomatic managements (antihistamines, topical steroids) can be used adjunctively. www.UpToDate.com Topics: Sabies
Mite eradication • Close contacts should be treated (symptomatic or not). • Recently used (previous 3 days) clothes, linens, stuffed toys should be placed in a plastic bag for at least three days OR machine washing with hot water and then ironing OR drying in a hot dryer, OR dry cleaning. Freezing at -20ºC for 24 hours is another option. www.UpToDate.com Topics: Sabies
Question #3 • By the time the average traveller presents for care of a scabies infestation, they re usually infested with: • Less than 20 mites • 20 to 200 mites • 200-2,000 mites • 2,000 to 10,000 mites • Over 1,000,000 mites
Fleas • Fleas are common insect ectoparasites of mammals and birds. • Live in the environment close to their hosts. • They are likely to be encountered by travellers. • Most important to travellers are the cat and dog flea, the human flea the chigoe flea and the oriental rat flea.
Cat, dog and human fleas • These are largely nuissanceectoparasites. • Lesions are pruritic, similar to insect bites. • Bites usually in areas within 30cm of the ground of infested environment. • Lesions may appear in clusters. • Travel-associated cases usually require on reassurance and symptomatic management. • Cat and dog fleas (Ctenocephalides) can transmit cat-scratch disease (Bartonella) and murine typhus.
Chigoe fleas • Tunga penetrans causes an ectoparasitic infection called tungiasis. • Endemic to South America, Central America, the Caribbean, Asia and Africa. • Prevalence amongst local inhabitants of some regions reaches 50%. • Infestation typically occurs on the feet. • The fertilized female burrows into the patient’s skin, its head toward the epidermal-dermal junction and its anal-genital opening near the surface. CMAJ March 14, 2006 vol. 174 no. 6 775-776
Tungiasis • Feeds on blood and enlarges to a pea-size, producing a whitish nodule with a central black dot corresponding to the anal-genital opening. • One to three weeks after penetration, the flea expels eggs from the central opening. • Approximately five weeks following penetration, the flea dies and is sloughed off, leaving an ulcer that heals slowly.
The oriental rat flea • Worldwide distribution (wherever there are rodents). • Most common host is rats. Opportunistic feeder on humans. • Creates lesions similar to other fleas but is an efficient vector for bubonic and septicemic plague.
Bubonic Plague • Most common form of plague • Papule or ulcer may be present at the site of inoculation. • Sudden onset of high fever, chills, and headache. • Painful, swollen lymph glands (buboes) arise, usually in the groin, axilla, or neck. • Area draining the inoculation site. • May progress to septicemic or pneumonic plague or spontaneously heal. • Somewhat contagious. • Contact with buboes.
Septicemic Plague • Organisms invades bloodstream and disseminates. • Buboes usually absent. • Abdominal pain, diarrhoea and vomitting common. • May progress to pneumonic plague. • Mortality extremely high. • Not very contagious without respiratory symptoms.
Pneumonic Plague • Most feared form of plague. • Incubation short (2 – 3 days) • Invasion of bacilli into the alveolar space. • Primary (inhalation) or secondary (bacteraemia) • High mortality. (>50-90%) • Highly contagious. • Transmission occurs within 2 metres.
Oriental rat flea • Xenopsyllacheopsishas global distribution and bites will occur in travellers. • Concern is where plague occurs either in humans or where plague is naturally carried by rodents. • Travellersand travel health experts should be aware where plague is occurring (outbreaks and natural) to provide targeted enhanced counselling. • Exposure to carrier animals (rats, other rodents) and their nesting areas should be avoided. • Prevention of arthrobod (flea) bites. • Avoid unprotected contact with plague patients.
Plague in madagascar • Between August and November 2017, over 2300 cases and 200 deaths occurred in Madagascar. • Plague is already endemic in Madagascar and tends to occur between September and April • The majority (76%) have been pneumonic (person-to-person transmission) while the remainder were bubonic (flea or animal associated). Only one case on septicemic plague was reported. • Pneumonic cases are typically acquired from an infected individual while bubonic cases are typically transmitted from an infected flea or by direct contact. • Aggressive public health measures effectively controlled the outbreak and no new cases have been reported since November. http://www.who.int/csr/don/27-november-2017-plague-madagascar/en/
Plague and travellers • Generally, travellers are not at risk of plague, but infection is possible. No travel associated cases have been reported in association with the Madagascar outbreak. • Travellers in rural areas of plague-endemic regions may be at risk, particularly if camping or hunting or if contact with rodents takes place. • Travellers to areas where pneumonic plague is emerging or who will have close contact with pneumonic plague victims are also at risk of acquiring pneumonic plague. • Travellersand travel health experts should be aware where plague is occurring (not just Madagascar!) to provide targeted enhanced counselling. • Exposure to carrier animals (rats, other rodents) and their nesting areas should be avoided. • Prevention of arthrobod (flea) bites. • Avoid unprotected contact with plague patients. http://www.who.int/ith/updates/20171003/en/
Fleas - management • Most are nuisance biting insects and management is supportive. • For tungiasis, nodule contents or entire lesion should be removed. Antibiotics should be given for secondary infections. Tetanus prophylaxis is indicated. Ivermectin may be effective but is not indicated unless there are numerous lesions. • Species that are vectors for disease (e.g. plague) are controlled by excluding rats from dwellings, using insecticides and exterminating rodents. • Flea treatment effective for domestic animals. • If exposure is inevitable, covering legs, using insecticide treated clothes and covering feet are very effective for all flea types. • Repellants may be partially effective. CMAJ March 14, 2006 vol. 174 no. 6 775-776
Ticks • Hundreds of tick species exist. • A relative few are important to humans and travellers. • Majority of tick bites are harmless or nuisance only. • Four major health issues arise from tick bites: • Allergic reactions. • Permanent allergies to mammalian meat. • Tick paralysis • Transmission of infections
Important ticks for travellers • Ixodesscapularis: Deer tick • Most of temperate Eastern North America. • Ixodesricinus: Castor bean tick • Most of Central Europe and Central Asia • Ixodesholocyclus: Queensland tick • Eastern Australia • Dermacentorvariabilis: Dog tick • Most of North America East of the Rockies • Amblyommaamericanum: Lone Star Tick • Southeast USA • Amblyommavariegatumand A. hebraeum: Tropical and South African bont ticks • Subsaharan Africa • Rhipicephalussanguineus: Brown dog tick • Global distribution (30ºS to 50ºN) Am J Clin Dematol 2009: 10(1): 1-8 Clin Microbiol Rev 2014 27: 48-67
Ixodes sp. • Black-legged deer tick: Transmits several disease to humans: • Borreliosis (Lyme, mayonii and miyamotoi), anaplasmosis, babesiosis, Powassan virus. • Castor bean tick: • Borreliosis(Lyme–like and others), Tick-borne encephalitis, Q-fever, Rickettsial disease (Bouttoneuse fever). • Queensland tick: • Rickettsial disease (Queensland tick typhus), borreliosis (lyme-like), mammal meat allergy, tick paralysis (severe form). Ticks Tick Borne Dis. 2018 Feb;9(2):354-362.
Dermacentor sp. • Dog tick (AKA Wood tick): • Rickettsial diseases (e.g. RMSF), tick paralysis (mild form), tularemia. Ticks Tick Borne Dis. 2018 Feb;9(2):354-362.
Amblyomma sp. • Lonestar tick: • Rickettsial diseases(eg.RMSF), Mammal meat allergy, STARI agent, ehrlichiosis, tularemia. • Bont ticks • African tick typhus Ticks Tick Borne Dis. 2018 Feb;9(2):354-362.
Question #4 • The majority of ticks found on humans in Manitoba are: • Black-legged deer ticks (Ixodesscapularis) • Dog ticks (Dermacentorvariabilis) • Gopher ticks (Ixodescookei) • Brown Dog Ticks (Rhipicephalussanguineus) • Lone star ticks (Amblyommaamericanum)
Flies and myiasis • Myiasis-causing flies occur globally, but are common in travellers to central and South America and Africa. • Infestation of human or animal tissues with the larvae of flies (“maggots”) • Human myiasis occurs in three forms: • Obligatory myiasis: Larvae feed on healthy tissue. • Facultative myiasis: Larvae feed on dead/diseases tissue of host. • Accidental myiasis: Incidental colonization or finding of larvae on humans.
Myiasis • Several sites can be implicated. • Furuncular myiasis (Skin) • Ophthalmomyiais: Internal or external eye • Urinary tract • Gastrointestinal tract • Oral and nasopharyngeal myiasis • Wound myiasis – May be obligatory or facultative myiasis. • Gross fact: Occasionally used therapeutically for debridement.
Furuncularmyiasis • Cased by obligatory ectoparasites whose larvae enter intact skin. • Most common causes are Dermatobia hominis (South and Central America) and Cordylobia anthropophaga (African Tumbu fly). • Other flies (Hypoderma spp., Cuterebra spp., Gasterophilus spp.) are distrubuted worldwide and associated with occasional cases of human myiasis.
Dermatobia • Dermatobia lays eggs on mosquitoes which drop them on human (and animal) hosts. • Usually a single lesion. • The larvae hatch from the egg, enter intact skin an mature over 2 – 3 weeks. • Larvae enlarge and create a furuncular lesion with small opening on surface for breathing. • At maturation, the larva drops out of the host, pupated and becomes adult. Clin Microbiol Rev 2014 27: 48-67
Question #5 • Explain why mosquito repellant is effective for the prevention of South American funruncular myiasis but completely ineffective for African furuncular myiasis.