Download
1 / 38
380 likes | 398 Views
This review provides the best evidence on managing various ENT emergencies seen in the ED, including epistaxis, fishbone foreign bodies, tonsillitis, and post-tonsillectomy epistaxis. It discusses interventions such as INR management, cool compress, topical antibiotics, hemostatic agents, and safety considerations for bilateral packing. The review emphasizes pearls for managing epistaxis, such as cautery techniques and the use of hemostasis agents like Floseal and Gelfoam. Additionally, it covers topics like the efficacy of fibrin glue, tranexamic acid, and antibiotic use with packing. The review also includes insights on fishbone foreign body management, emphasizing the utility of imaging studies and when to involve ENT specialists.

E N D
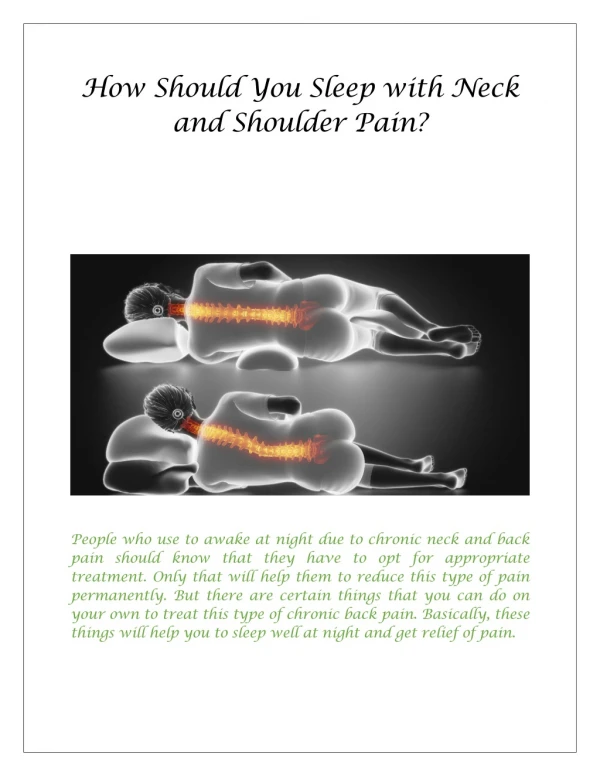
Pain in the Neck!An EBM review of emergency department ENT Petr Balcar FRCPC Dec 15, 2011
Outline • Review best evidence in management of • Epistaxis • Fishbone FB • Tonsillitis • Post Tonsillectomy
Epistaxis Questions • Discuss evidence for: • INR • Cool compress • Topical antibiotics • Hemostatic agents • Oral antibiotics in packing • Safety of bilateral packing
Epistaxis: Pearls • Speculum parallel to floor! • Cauterize • Only controlled bleed • Periphery inward • 1cm around bleeder • Wipe excess AgNO3 off • Rapid Rhino • No saline/vaseline • Impairs mesh thrombosis • Recheck cuff 10-15min
Epistaxis: Anticoagulation • Not routine • Warfarin with therapeutic INR • 25% annual rate • Rare to need reversal • Discussion point: • Do all need ENT FU?
Epistaxis: Cool Compress • BestBets review • 3 small studies: • 1. Sucking ice = nasal vasoconstriction • 2. Neck ice packs = nasal vasoconstriction • 3. Forehead ice = 22/28 bleeds stopped • Summary: • Scant evidence • Benign intervention • Discussion point: • Should we hand out ice at triage? • Anyone want to do study?
Epistaxis: Topical Antibiotics • Multiple pediatric studies • Intranasal antibiotic x 4wks = cautery • No long term benefit • Minimal sefx • Staph carriage in adults • Walker and Baring 2009 • Small RTC n=49 • Nasal swabs • No difference in S. aureus carriage ~21% • Conclusion • Consider in pediatrics
Epistaxis: Hemostasis Agents • Multiple thrombogenic products • Quixil (fibrin glue spray) • Floseal (thromin gel) • Surgicel • Gelfoam • Avitene • Positive effect in small studies, few RCTs • Primarily developed for surgical use
Epistaxis: Fibrin Glue • Vaiman 2002 • RCT n 204 • Fibrin glue (Quixil) vs AgNO3 vs Cautery vs foam packing • ~93% immediate cessation • Mean 2.5 min • Fewer mucosal sefx
Epistaxis and Tranexamic Acid • Lysine derivative • Antifibrinolytic • Prevents plasmin to plasminogen • Hereditary hemorrhagic telangectasia • Case studies • Benefit of intranasal spray • Cochrane study under way
Epistaxis: Antibiotics with Packing • Postoperative rates 16 : 100,000 • PO antibiotics do not reduce nasal staph • No good studies: very rare event • Multiple side-effects of antibiotics • Most ENTs do it • Higher risk elderly, immunocompromised, prolonged pack • Discussion Point: • Do you start antibiotics?
Epistaxis: Bilateral Packing • Hollis 2011 • Anatomical model • Bilateral pack = decrease in septal deflection • Hady 1983 • Healthy volunteers packing • ABG at 24 hrs • Increased CO2, decreased PO2, pH equal • Loftus 1994 • 19 pts, posterior pack • Pulse oximetry monitor x 1200hrs • No desats
Epistaxis: Bilateral Packing • Historical cases with bad outcomes • Posterior packing patients died • Hypothesized nasopulmonary reflex • No current evidence of significant morbidity/mortality with bilateral packing • Posterior bleed patients need admit • Anterior bleed with bilateral pack • Consider DC in healthy patients, admit in frail/elderly • Discussion point: • Who does bilateral packing? • Do you admit them?
Fish Bone: Questions • How useful is plain X-ray? • How useful are symptoms? • Do all need scope?
Fish Bone: Are Bones Opaque? • Lue 2000 • 10 fish bones in cadaver head/neck • Blinded radiologists • Plain Xray 39% sensitive • CT 9/10 found • Cooking did not change opacity • Variability by species, orientation • Hone1995 • 10 fish bones in cadaver neck • 9/10 seen by both rads
Fish Bone: Clinical Xray Utility • Several clinical imaging studies • Sensitivity ~30% • Specificity ~88% • Ngan 1990 • Prospective n=358 • Clinical symptoms not reliable for FB • Clinical symptoms did localize FB if present • 117 bones found • 21 direct removal • 82 endoscopic removal
Fish Bone: Clinical Relevance • Impacted oropharyngeal bone location • Tonsils, base of tongue, vallecula • Impacted bones migrate! • Many case reports of significant pathology • Abscess, vascular • Should not be ignored! • Discussion point: • Do you xray all patients? • Do you get ENT/GI FU for all patients?
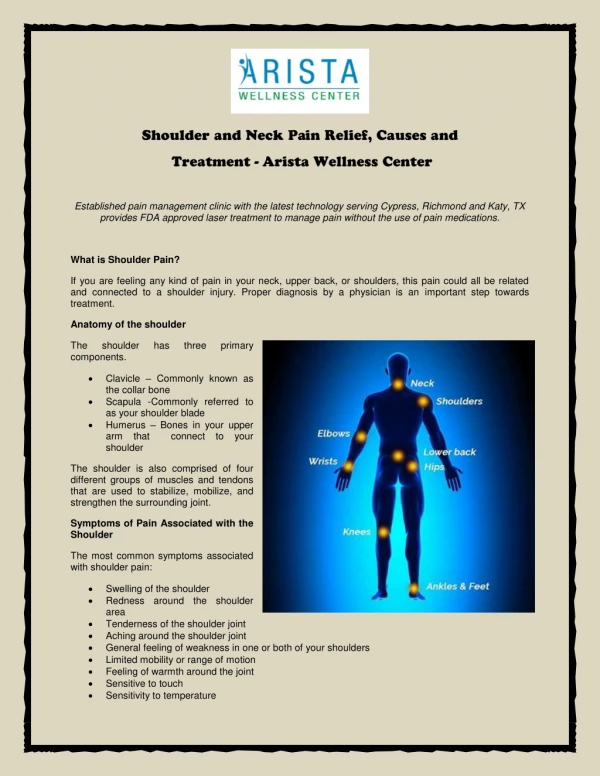
Pharyngitis: Questions • Review pathogens • Best evidence: • When to treat • Which antibiotics and how long • What to do if treatment fails • Analgesia
Pharyngitis: Bug Pearls • Usually viral • Consider EBV • GAS • Very common • Serious Complications • GBS/GCS minimal complications • HIV in at risk population • Early diagnosis/treatment • Mycoplasma / Chlamydia • Peds RCT n=133 • >30% carriage, not improved by Azithro • Ghonococcal • 5-15% carriage in MSM • Rare symtomatic, Rc Ceftriaxone • Diptheria • Un-immunized, endemic travel
Pharyngitis: Why Treat GAS? • Prevent complications • Suppurative • Rheumatic Fever • Up to 9 days post ssx • Scarlet Fever • Reduce symptoms • If within 48hrs • Reduce transmission • ~35% close contacts • Within 24hr, 80% swab neg
Pharyngitis: Antibiotics • Penicillin • 100% susceptibility • Pen V PO x 10days • Pen G IM lasts 3-4 weeks! • Amoxicillin • 100% susceptibility • Tastes better (yum) • AOM 15% • Clindamycin • 93% susceptibility • Better staph/anaerobe
Pharyngitis: Antibiotics • Cephalosporins • 100% susceptibility • Casey et al 2004 • Meta analysis: pen vs cephalosporin • <18yrs, n=7135 • Clinical and culture cure • Both superior in cephalosporins • Cost more, increased use in community • Macrolides • 93% susceptibility • Meta analysis shows improved compliance
Pharyngitis: Why Antibiotics Fail • Confirmed GAS • Chronic Carrier (up to 20% peds) • Poor compliance • Re-infection • Pet, toothbrush, dentures • Other beta-lactamase flora • Poor antibiotic penetration of tissue • Resistant strain (No pen resist strain Identified!) • Treat too early, reduced immune response • Non GAS • Suppurative complication
Pharyngitis: When Treatment Fails • No Specific Evidence • Screen for atypical etiology • Look for abscess • Repeat culture GAS + • Consider other PO Abx +/- IM Pen • Recurrent episodes • Consider testing family and treat all +ve • Consider chronic carrier with Viral • 6/year = tonsillectomy
Pharyngitis: Evidence for Steroids • All ENT’s do it! • Cochrane study in progress • Multiple small studies • Pediatrics • 3 studies • Oral Dexamethason • Adults • 7 studies • IM or PO steroid • Overall ~ 5-6hr quicker pain relief • No Early difference in Sefx
Pharyngitis: Summary • Consider atypical causes • High risk: tearly + swab • Antibiotics • Penicillin still 1st choice • Cephalosporins excellent • Amoxil peds • Failure re-test • Analgesia • Topical lozenges • Steroids
Peritonsillar Abscess: Questions • Utility of US • Best treatment options
Peritonsillar Abscess: US Imaging • Relatively new • Several small studies • Excellent for Abscess locations • Intraoral = 95% sensitive • Transcutaneous = 80% sensitive
Peritonsillar Abscess: US Drainage • Costantino 2010 • RCT n=23 • ED physician, US vs blind drainage • Diagnosis 100% vs 63% • Aspiration 100% vs 42% • ENT Referal 8% vs 55%
Peritonsillar Abscess: Treatment • Several poor studies • Overall I&D = Needle • ~90% success rate • Consider primary tonsillectomy • Antibiotics • Usually polymicrobial • IV Pen/Clinda • PO Pen/Clinda/Amox-clav • Steroids reduce morbidity
Peritonsillar Abscess: Summary • Needle okay • US guided probably best • Iv steroid dose helps • Discussion point: • Lets buy an oral probe!
Post Tonsillectomy: Questions • Indications • How much bleeding is concerning? • Analgesic options
Post Tonsillectomy: Bleeding • Significant hemorrhage 1-3% • 1:40,000 fatal • 95% secondary (>24 hr) • Up to 39 days • Blood = ENT • Consider admit • Active bleed • Pressure • Epi • +/-Thrombin
Post Tonsillectomy: Analgesia • Expected pain pattern: • Improve over 3-5 days • Then increases for 1-2 days • Resolves • Steroids given periop • NSAIDS?
Post Tonsillectomy: NSAIDS • Surgeon will not be pleased! • Several RCTs, 2 good reviews • Marret 2003 • N = 262 • Need for OR • NNH 29 • Moinche 2003 • N = 970 • Need for OR • NNH 60 • Reduction in N/V vs opioid • NNT 9
Post Tonsillectomy: Summary • Delayed pain presentation • Any bleed need ENT FU • No NSAIDs
References • Alcaide, ML et al. Pharyngitis and Epiglottitis Infect Dis Clin N Am. 2007 21:449-469 • Altamimi S, Khalil A, Khalaiwi KA, Milner RA, Pusic MV, Al Othman MA. Short versus standard duration antibiotic therapy for acute streptococcal pharyngitis in children. Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD004872. DOI: 10.1002/14651858.CD004872.pub2 • Casey JR and Pichichero ME. Meta-analysis of cephalosporin versus penicillin treatment of group A streptococcal tonsillopharyngitis in children. Pediatrics 2004 Apr; 113:866-82. • Costantino, TG et al. 224: A Prospective, Randomized Comparison of Ultrasonography-Guided and Non Ultrasonography-Guided Peritonsillar Abscess Drainage by Emergency Physicians. Annals of Emerg Med. 2010. 56(3supl); s74 • Fisher, J et al. Efficacy and tolerability of ambroxol hydrochloride lozenges in sore throat. Randomised, double-blind, placebo-controlled trials regarding the local anesthetic properties. Arzneimittelforschung. 2002;52(4):256-63. • Galioto, NJ. Peritonsillar abscess. Am Fam Physician. 2008 Jan 15;77(2):199-202. • Gerber, MA. Diagnosis and treatment of pharyngitis in children. Pediatr Clin N Am. 2005. 52:729-747 • Herzon FS, Martin AD. Medical and surgical treatment of peritonsillar, retropharyngeal, and parapharyngeal abscesses. Curr Infect Dis Rep. 2006;8(3):196–202. • Lue, AJ et al. Use of plain radiography and computed tomography to identify fish bone foreign bodies. Otolaryngol Head Neck Surg 2000. Oct 123(4); 435-8 • Marret E, Flahault A, Samana C M, Bonnet F. Effect of Postoperative, Nonsteroidal, anti-inflammatory Drugs on Bleeding Risk after Tonsillectomy. Meta-analysis of Randomised, Controlled Trials. Anesthesilogy 2003;98(6):1497-502. • McIsaac WJ et al. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ 1998;158(1):75-83. • McIsaac WJ et al. The validity of a sore throat score in family practice. CMAJ. 2000;163:811–5. • Moiniche S, Romsing J, Dahl J B, Tramer M R. Nonsteroidal Antiinflammatory Drugs and the Risk of Operative Site Bleeding After Tonsillectomy: A Quantitative Systematic review. Anesth Analg 2003;96(1):68–77.
References cont • Ngan, JH et al. A prospective study of fish bone ingestion. Experience of 358 patients. Annals of Surgery 1990. 211(4);459-62 • Nitu, IC et al. Clinical experience with the use of clotting factor concentrates in oral anticoagulation reversal. Clin Lab Haematol 1998. 20:363Pichichero ME. Systematic review of factors contributing to penicillin treatment failure in Streptococcus pyogenes pharyngitis. Otolaryngol Head Neck Surg 2007. Dec 137(6): 851-857. • Porter MJ. A comparison between the effect of ice packs on the forehead and ice cubes in the mouth on nasal submucosal temperature. Rhinology. 1991 Mar;29(1):11-5 • Vincent MT et al. Pharyngitis. American Family Physician 2004. Mar 15;69(6):1465-1470 • Walker, FDL and DE Baring. Nasal bacterial carriage in adult epistaxis: is neomycin the answer? J of laryngology and Otology. 2009 JUN 123(6): 623-5 • Wing et al. Effectiveness of Corticosteroid Treatment in Acute Pharyngitis: A Systematic Review of the Literature. Acad Emergency Medicine 2010. 17(5):476-483. • Wonnemman, M et al. Lidocaine 8 mg sore throat lozenges in the treatment of acute pharyngitis. A new therapeutic option investigated in comparison to placebo treatment. Arzneimittelforschung 2007; 57(11) :689-97. • www.Bestbets.org. (2011). Anterior epistaxis - does cooling decrease bleeding? Retrieved Nov 28, 2011 from http://www.bestbets.org/bets/bet.php?id=568 • www.Bestbets.org. (2011). Lateral neck x-rays are not indicated in the emergency department management of suspected fish bone impaction. ? Retrieved Nov 28, 2011 from http://www.bestbets.org/bets/bet.php?id=29 • www. clinicalevidence.bmj.com. (2011). Nosebleeds in children. Retreived Nov 28, 2011 from http://clinicalevidence.bmj.com/ceweb/conditions/chd/0311/0311_I1.jsp • www.emedicine.medscape.com (2011). Tonsillectomy treatment and management. Retreived Dec 2, 2011 from http://emedicine.medscape.com/article/872119-treatment#a17 • www.uptodate.com (2011). Treatment and prevention of streptococcal tonsillopharyngitis. Retreived Nov 28, 2011 from http://www.uptodate.com/treatment-and-prevention-of-streptococcal-tonsillopharingitis