Download
1 / 49
570 likes | 992 Views
INGUINAL HERNIAS. The term “inguinal hernia" is applied to those hernias which traverse the inguinal canal to emerge at the external abdominal ring, Depending on the exact site of the aperture two varieties are recognized, the oblique and the direct. Surgical anatomy The Inguinal Canal:

E N D
The term “inguinal hernia" is applied to those hernias which traverse the inguinal canal to emerge at the external abdominal ring, Depending on the exact site of the aperture two varieties are recognized, the oblique and the direct
Surgical anatomy • The Inguinal Canal: • It is oblique & directed downwards, forwards & medially • It has the following boundaries: • I. Anteriorly:External oblique aponeurosis (EOA) & lateral fibers of internal oblique (lateral 1/2) • 2. Posteriorly:Transversalis fascia & conjoint tendon (medial 1/2) & reflected ligament (medial 1/4) • 3. Superiorly:Arched fibers of the internal oblique muscle • 4-Inferiorly:Base of the inguinal ligament (Poupart's ligament) & pectineal ligament
The Inguinal Rings: • Superficial Inguinal Ring (SIR):Opening in the external oblique aponeurosis (EOA)& lies just above the pubic tubercle & transmits the spermatic cord • Deep Inguinal Ring (DIR):Opening in the fascia transversalis & lies 1/2 an inch above the mid inguinal point (lateral to the inferior epigastric artery, lEA)
Fascia Transversalis: • • It is part of the endoabdominal fascia enclosing the abdominal cavity, deriving its name from the overlying transverses abdominis muscle • The fascia transversalis is continuous with the following: • AboveDiaphragmatic fascia • BelowPelvic fascia - anterior femoral sheath • PosteriorFascia iliacus - renal fascia
Parts of the fascia transversalis: • Henel’s ligament: Thickening of the extreme medial portion of fascia transversalis in conjunction with the pubic insertion of rectus abdominis tendon • Hasselbach's ligament:Lies just medial to the internal ring. It strengthens the medial margin of the ring • Rectus fascia:Fascia transversalis divides medially to invest the rectus abdominis muscle • Iliopubic tract:Attached laterally to the anterior superior iliac spine and medially to the pubis
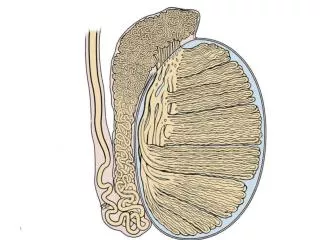
The Spermatic Cord: • Coverings: • Internal spermatic fasciaderived from the fascia transversalis, at the DIR • Cremasteric muscle & fasciafrom the internal oblique muscle • External spermatic fascia derived from the external oblique aponeurosis at the SIR
Contents: • Vas deferens • Arteries:Testicular artery (internal spermatic) - cremasteric artery (external spermatic) - artery of vas • Veins:pampiniform plexus of veins (which form the testicular veins that end in the left renal vein on the left side and the IVC on the right side) • Lymphatics of the testis • Nerves:Sympathetic fibers from the hypogastric plexus - Genital branch of the genito-femoral nerve
Normal Protective Mechanisms Against Inguinal Herniation: • Shutter Mechanism:On straining, the arched fibers of the internal oblique muscle & conjoint tendon descend downward while the inguinal ligament ascends upward to obliterate the gap in between • Plugging Mechanism:On straining, the cremasteric muscle contracts upward taking with it the spermatic cord & plugs the DIR
Sliding Mechanism:On straining, the deep inguinal ring becomes "slit-like" because it is pushed up & laterally by the action of the transversalis fascia • Valvular Mechanism:On straining the AW approximates the PW, thus occluding the canal • Obliquity of the Inguinal Canal:It is 3.75 cm in length extending from the DIR to the SIR, and contains the spermatic cord or round ligament of uterus, ilio-inguinal nerve (overlies the cord in the canal) & lymphatics
The integrity of fascia transversalis • Weak parts are opposed by strong parts e.g. ant wall of the inguinal canal in front of internal ring and posterior wall of the inguinal canal is strong behind the external ring • Physiological Tendency to do the acts of increase intra-abdominal pressure in the squatting position so approximating the anterior wall of the canal to the posterior wall
Myopectineal orifice (MPO) of Fruchaud • Anatomic hole located between the false pelvis and ipsilateral lower extremity • This is a weak area in the groin where posterior layer is not protected by overlying muscle • The myopectineal orifice is quadrangular in shape and is divided into a superior and inferior level by the inguinal ligament • Its role is to allow passage of the spermatic cord structures superiorly and the femoral vessels inferiorly
The boundaries of the myopectineal orifice are the arching fiber of the internal oblique superiorly, the rectus abdominis muscle medially, the anterior borders of the iliac bone inferiorly, and the iliopsoas and iliopectineal arch laterally • This anatomic hole can be further divided into 3 anatomic triangles (medial, lateral, and femoral), which are potential sites of groin herniation
The medial triangle is the space encircled by the arching fibers of the internal oblique superiorly, the rectus abdominis medially, the inguinal ligament inferiorly, and deep epigastric vessels laterally • This medial triangle within the myopectineal orifice is the site of direct herniation within the groin
The next anatomic triangle within the myopectineal orifice is the lateral triangle • The triangle is defined by the deep epigastric vessels medially, the inguinal ligament inferiorly, and a line drawn from the lateral inguinal ligament to the intersection of the deep epigastric vessels with the arching fibers of the internal oblique
The final triangle within the myopectineal orifice is the femoral triangle • Located in the inferior aspect of the myopectineal orifice, the area is bordered by the Cooper’s ligament inferiorly, the inguinal ligament and iliopubic tract superiorly, and iliopsoas muscle laterally
All groin hernias begin as a weak area in the myopectineal orifice • The transversalis fascia layer deteriorates and allows a peritoneal protrusion through it • Depending on the length of the insertion of the transversusabdominis on the Cooper's ligament, the presence of a patent processus vaginalis, and the size of the femoral ring, the hernia can be direct, indirect, femoral, or any combination of the three • Groin hernia can be corrected by either repairing all or part of this myopectineal orifice or by substituting a prosthesis for the deteriorated transversalis fascia
Etiology • Most oblique hernias in children and young adults occur into“Preformed sacs”which represent a partially or completely patent processusvaginalis • In old age, most cases are due to the formation of a “pulsion sac”as a result of muscular weakness and raised intraabdominal pressure
Anatomical Types: The common varieties are Funicular:The tunica vaginalis is normal, and the sac represents the proximal portion of the processusvaginalis only Infantile:The tunica vaginalis extends upwards towards the internal ring so that the sac passes down behind it. At operation, the tunica is liable to be opened in mistake for the true sac which will be found behind it Congenital:The whole processus is patent so that the sac is continuous with the tunica vaginalis and the testis lies among the contents. Though called congenital, it may not appear until adolescent or adult life
Interstitial:This type occurs most often in association with undescended testis where the sac passes between the layers of the abdominal wall instead of descending into the scrotum. It may pass: • Between the peritoneum and transversalis fascia (properitoneal type); (b) Between the internal and external oblique (intraparietal type); or • c) Between the skin and external oblique (proparietal type) • Sometimes, the hernia starts with an ordinary sac which becomes obstructed at the external ring so that it extends between the muscles as a bilocular sac (hernia-en-bisac)
Saddle-bag: • There are two sacs, direct and indirect, separated by the deep epigastric artery, hence the term “pantaloon hernia" • At operation, the direct sac is drawn lateral to the deep epigastric vessels by traction on the oblique sac so that the two sacs are converted into one
Sliding (hernia-en-glissade): • This variety is especially common in elderly patients with longstanding large hernias • The sac enlarges by drawing on the posterior parietal peritoneum covering the caecum or pelvic colon which passes through the inguinal canal outside the sac • At operation, it is impossible to separate the sac from the bowel which should, therefore, be elevated with a fringe of sac by making a U-shaped incision around the bowel and closing it longitudinally
Clinical Features • Incidence: • Oblique inguinal hernia accounts for about 70% of all hernias • It is commonest in infants, children and young adults, and in about 30% of cases both sides are affected • Males are affected at least 20 times more often than females, and the hernia is slightly commoner on the right side, probably due to the later descent of the right testis
Symptoms: • The patient complains of pain and intermittent swelling at the groin, which appear during standing, coughing, straining or exercise and disappear on lying down • Signs: • The swelling may be limited to the groin (buboncele) or may reach the scrotum (scrotal hernia) • The following signs can be elicited: • Expansile impulse on coughing
Reducibility • In an upward, then outward and finally backward direction, by gentle squeezing over the fundus • Descent • In the opposite direction on standing or coughing after reduction • Internal ring test:Pressure with the thumb over the internal ring after reduction, prevents descent of the hernia and abolishes the expansile impulse on coughing
External ring test: • Normally, the external ring does not admit the tip of the little finger. In inguinal hernias, it becomes wide enough to admit the tip of the finger by invaginating the scrotal skin. If the patient with an oblique hernia is asked to cough while the finger is inside the canal, the expansile impulse will be felt at the tip of the finger, whereas in a direct hernia it will be felt at the back of the finger
Consistency:An enterocele is soft and resonant on percussion but an epiplocele feels doughy and dull • Relations:The pubic spine lies to the inner side of the swelling with Poupart's ligament below and laterally and the vas below and medially. Except in the congenital variety, the testis can be felt distinctly at the lower and back part of the swelling • Transillumination:The swelling is always opaque on transillumination, but in infants and children it may be semitranslucent
Operative treatment • Herniotomyis suitable only in children and young adults provided the aperture is small and the abdominal muscles are strong • Technique: • An incision is made one-finger breadth above and parallel to the medial two-thirds of the inguinal ligament • The external ring is exposed and the external oblique aponeurosis is incised in the line of its fibers to open the inguinal canal from the external ring to the level of the internal ring
The cord is then hooked on the finger and held up in a ring forceps or over a strip of gauze • The coverings are incised longitudinally, taking care not to injure the ilio-inguinal nerve • The sac usually lies anterior to the structures of the cord and can be readily identified by its pearly white color • The coverings are separated by blunt dissection until the fundus of the sac is seen • The edge of the fundus is caught by artery forceps and separation of the sac is continued until the neck is exposed, as indicated by the adherent condensation of fat and the presence of the inferior epigastric vessels at its medial side
The sac is now opened at the fundus and any adherent contents are separated and returned to the abdomen • The sac is next twisted to narrow its neck which is transfixed and ligated with chromicized catgut as high as possible • The sac is then excised about 1 inch distal to the ligature, and the coverings of the cord are approximated with fine plain catgut • The cord is allowed to fall back into the canal, and the external oblique is repaired by interrupted sutures of chromicized catgut until the external ring fits snugly around the cord • After careful haemostasis, the subcutaneous fat is approximated with fine plain catgut, and the skin is closed with interrupted silk
Herniorrhaphy:In older patients and large or longstanding hernias, the inguinal canal should be repaired after complete excision of the sac • Bassini's operation • Is the standard method • The lower border of the conjoined tendon is sutured to the inguinal ligament behind the spermatic cord by means of 4 or 5 sutures of non-absorbable suture. If the sutures are tied under tension because the gap is wide, a Tanner's release incision should be made into the anterior rectus sheath so that the sutures do not cut out. The drawback of the operation is that it abolishes the “Shutter mechanism” of the inguinal canal by interfering with the action of the conjoined tendon
Halsted's operation • May be carried out as an alternative to Bassini's method in very large or recurrent hernias, especially in elderly and obese patients • In this method, the Bassini repair is reinforced by overlapping the aponeurosis of the external oblique behind the cord which becomes subcutaneous • It is an excellent method but since the cord runs directly through the muscles near the midinguinal point, the inguinal canal is no longer oblique and its valvular mechanism is lost
Bloodgood’s operation • Is preferred by some surgeons because it preserves both the shutter and valvular mechanisms • The posterior wall of the canal is strengthened by means of a triangular flap of anterior rectus sheath which is turned downwards at its lateral border and sutured to the inguinal ligament behind the cord
Freeing the cuff of transversalis fascia from the spermatic cord at the internal ring. Note the cremasteric tissue lies intact on the canal floor but is being freed at the internal ring
Splitting of the transversalis fascia from the internal ring to the pubic crest as far as desired
First suture line continues to tack the lateral flap of transversalis fascia to the transversalis fascia lying medially beneath the rectus, transversusabdominis, and internal oblique muscles
Reconstruction of the internal ring incorporating transversalis fascia and the proximal stump of cremasteric muscle
Second suture line ‘‘carrying’’ the previous established medial flap of tissue to the curved or shelving edge of the inguinal ligament
Complete groin repair sutures being placed through the defect to pick up Cooper’s ligament, then back out anterior and superficial to the iliopubic tract and inguinal ligament, in wide, loose loops
The nylon darn repair He described a repair using nylon suture material as a two-layered darn in an attempt to obtain a tension-free lattice to reinforce the transversalis fascia and surrounding tissues
Imbrication/plication of a direct sac to flatten the floor of the inguinal canal
Inverting the unopened indirect sac, having freed the margins of the neck completely at the deep ring
Placing a mesh cone in the deep ring. Insert: the cone in the deep ring
Mesh placement and attachment. The attachment must be wide enough to ensure that it can be tucked well up under the superior leaf of the external oblique and that its lower edge reaches or overlaps Poupart’s ligament. It is attached with a loose continuous suture. The infero-medial corner of the mesh (not shown) is secured to the soft tissues overlying the pubic tubercle with a 2- or 3-cm overlap
Tails of the mesh encircling the spermatic cord. One or two sutures are placed where the tails of the mesh cross lateral to the cord to ensure a snug fit