Download
1 / 56
570 likes | 732 Views
Anaemia; transfusion cases Therapeutics SAHD. Medical Students (Dr N Jackson) January 2011. Case 1. A 60-year old woman is noted to be pale and an FBC is performed: Hb 5.5g/dL; MCV 51.4fL WBC 6.9x10 9 /L; Plts 521x10 9 /L What is the likely diagnosis?

E N D
Anaemia; transfusion cases Therapeutics SAHD Medical Students(Dr N Jackson) January 2011
Case 1 • A 60-year old woman is noted to be pale and an FBC is performed: • Hb 5.5g/dL; MCV 51.4fLWBC 6.9x109/L; Plts 521x109/L • What is the likely diagnosis? • On what points will you major in the history? • What will you look for on examination? • What further tests will you request? • What treatments will you consider?
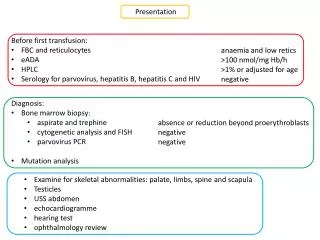
Case 1: Microcytic anaemia in a 60-year old woman • Likely diagnosis: Fe deficiency • History: • Intake (diet: …) • Blood loss (sites: …) • Malabsorption (history? test …) • Examination: GI • Further tests: (Ferritin); film; GI; TTG
Fe deficiency blood film So what treatment, and for how long? And what advice?
Case 1: Microcytic anaemia(Hb 5.5) in a 60-year old woman • Treatment (of Fe deficiency) • FeSO4 200mg OD TDS • Add vit C ? • 6/52 to restore Hb; 3/12 to replete • Dietary advice • What side effects to expect and how to avoid?
Iron therapy: side effects • GI – nausea, vomiting, epigastric pain, diarrhoea, constipation. • (Care in inflamm bowel dis, strictures, diverticular dis) • Black stools. • ?Take with food; build up dose slowly • Use lower Fe content preparations: • e.g. Ferrous gluconate 300mg TDS
No response to oral Fe? • Hb 6.5g/dL after 4 weeks treatment • What reasons can you think of?
No response to oral Fe? • Hb 6.5g/dL after 4 weeks treatment. • What reasons can you think of? • Non compliance • Non absorption (e.g. coeliac, small bowel resection) • Loss > absorption (i.e. bleeding ++) • What other treatment could you consider?
Parenteral Fe • Intramuscular: • Fe dextran • Intravenous: • Fe dextran = Cosmofer (TDI) • Fe sucrose = Venofer (x3/wk) • Fe carboxymaltose = Ferinject (TDI) • Fe isomaltoside = Monofer (TDI) • What are problems with this approach?
Parenteral Fe: side effects • IV infusion – ward, nurse time, cost • Allergic/anaphylactic reactions • Test dose may be required • Other infusion reactions (flushing) • GI symptoms • Headache • Taste disturbance Any questions on Fe therapy?
Case 2 • A 50-year old single man presents with fatigue. He admits to disliking vegetables. O/E: pallor; tinge jaundice; spleen tip palpable. • Hb 5.6g/dL; MCV 125fLWBC 3.0x109/L; Plts 80x109/L • Describe the abnormalities in the FBC. • List your provisional and differential diagnoses. • State the investigations you would request. • What treatment would you give while waiting for results?
Case 2 • Pancytopenia with macrocytosis: • Megaloblastic anaemia (B12/Folate) • Myelodysplasia • Acute leukaemia • Aplastic anaemia • EtOH/liver disease • Which of these would you favour?(NB dislikes vegetables) • Which investigations? (and expected results)
Case 2: Pancytopenia with macrocytosis • Most likely megaloblastic anaemia due to folate deficiency. • Investigations: • Blood film: oval macrocytes, aniso/poikilo hypersegmented neutrophils.(dysplastic features, blasts) • B12 & Folate(serum or RBC?) • ?Bone marrow: megaloblastic change
Megaloblastic Anaemia: blood film Before B12/Folate levels known, what treatment(s) would you give?
Case 2: Pancytopenia with macrocytosis • Treatments: • B12: Hydroxycobalamin 1000µg x5 …. • Folic acid: 5mg OD • Would you give Fe as well?If so, why? • If the results showed very low folate and normal B12; any further investigations?
Case 2: (cont’d) • The patient receives a course of treatment and soon feels much better, but his blood count is then: • Hb 9.0g/dL; MCV 64fLWBC 8.0x109/L; Plts 180x109/L • What complication has arisen, and why?
Case 2: (cont’d) • Complication? • Fe deficiency • Why? • Response to B12/Folate outstrips Fe stores • Many causes of B12/Fol deficiency also cause Fe deficiency. • What investigation & treatment? • No investigation – just give Fe.
Treating Folate deficiency • Do not use folates alone in unsorted megaloblastic anaemia: • In B12 def, may precipitate neurological problems • Use B12/Folate (+Fe) together in megaloblastic anaemia • Folic acid: 5mg/day ( if malabsorption present) • Prevention of neural tube defects: 400μg/day (low risk); 5mg/day (high risk) • Diet:beans, citrus fruits, dark green leafy vegetables, whole grains, poultry, pork, shellfish and liver • Think of cause: diet, malasorption (TTG) • Side effects: very rare.
Case 3 • A 49-year old man complained of lethargy and leg pain. He had undergone several blood transfusions but had become anaemic again.PMH: HypothyroidismO/E: very pale; no organomegaly; no CCF • Hb 2.1g/dL; MCV 114fLWBC 1.5x109/L; Plts 35x109/L • List your differential diagnosis. • What will you look for in the blood film (report)? • What further tests will you request? • What is your immediate treatment?
Case 3 • Differential diagnosis?(from the abnormalities in the FBC?)
Case 3 • Severe pancytopenia with macrocytosis (order re-arranged): • Acute leukaemia • Myelodysplasia • Megaloblastic anaemia (B12/Folate) • Aplastic anaemia • EtOH/liver disease • What will you look for in the blood film? And what other tests will you request?
Case 3: Pancytopenia with macrocytosis (severe) • Blood Film: • Leucoerythroblastic change ( diff ….) • Blasts • Dysplastic features (e.g. …..) • Oval macrocytes; hyperseg neuts • Other tests: • Bone marrow • B12, Folate • What will be your treatment while awaiting test results? Remember:Hb 2.1g/dL; MCV 114fL, WBC 1.5x109/L; Plts 35x109/L
Case 3: Pancytopenia with macrocytosis (severe) • Treatment while waiting tests: • Red cell transfusion • Bone marrow again turned out to be megaloblastic, with very low B12: • What neurological signs would you look for in the legs? • B12 <60ng/L. What further tests?
Subacute combined degeneration of spinal cord due to B12 deficiency
B12 deficiency • Main cause: pernicious anaemia • GPC or IF auto-ab. (Schilling test: no longer) • Rare: strict vegan diet, gastrX, terminal ileum removal, other malabsorption • Treatment = B12 • Hydroxycobalamin 1000µg IM x5 over 2/52, then 1000µg IM every 3/12 • Cyanocobalamin PO (if dietary cause) 50µg/day • Side effects rare : allergy; K+ initially
Part II: Transfusion cases
Case 1: Pre-op assessment • A 45-year old woman with fibroids has menorrhagia and is scheduled for a hysterectomy • In the pre-anaesthetic assessment clinic (PAAC): • Hb 8.9g/dL, MCV 73fL (WBC, plts normal) • Regarding her blood transfusion requirements, what action(s) will you take?
Case 1: Pre-op assessment: Microcytic anaemia • Hb optimisation ; oral Fe pre-op and recheck Hb/MCV. Diet, medical treat? • Transfusion information/consent • Blood ordering: MSBOS • Consider use of Cell salvage if predicted peri-op blood loss>1 L
Case 1. Peri-op transfusion • Hb 11.5g/dL pre-op as a result of Fe • ‘Group & Screen’ requested. • Patient Group: A Pos.Antibody screen: Negative • Patient said to be:‘suitable for electronic issue’.What does this mean?
Electronic issue • Two transfusion samples at different times; both showing same ABO/Rh group and negative Ab screen • ABO-compatible can be issued off the shelf without a crossmatch (10 mins). • More efficient use of blood.
Case 1 • Quite a lot of bleeding peri-op • Post-op Hb 7.8g/dL; patient feels well. • Will you prescribe blood transfusion? • If so, how will you do it?
Case 1. • If patient well and progressing post-op OK, then no need to transfuse. • (Indication is Hb<8 AND symptoms) • If prescribe blood: • Ring Blood Bank to order (from G&S) • Give in the day time (not after 10pm) • 1.5 hours per unit • No need diuretic in fit 45-yr old woman
Case 2. Liver biopsy • 45-year old woman with abnormal liver function (?cirrhosis) is due a liver biopsy • Blood count: • Hb 12.0g/dL, WBC 3.4x109/L, Plts 80x109/L • Coagulation screen: • PT 17 (control 14, INR 1.5), aPTTR 1.4 • Your SpR asks you to order appropriate blood products to cover the procedure. • What do you request?(Where would you look for advice?)
‘Policy for the transfusion of platelets, fresh frozen plasma and cryoprecipitate’ Answer: ensure vitamin K has beengiven.How should it be given? How long does it take to act?What are the side effects of vitamin K?
The side effects of vitamin K • Vitamin K-dependent clotting factors will take 18-24 hours to normalise • Minimal S/E. Should be given slow IV. • Occasional irritation at injection site • Oxidant drug – care in G6PD deficiency (-> haemolysis) • Oral vitamin K currently not available (use IV prep orally)
Case 2. Liver biopsy • Despite this, your registrar insists on giving 2 units of Fresh Frozen Plasma (FFP) immediately pre-biopsy. • The biopsy is carried out • Two hours later: Severe SOB and hypoxaemia (SaO2 78% on air) • CXR
Post Liver Bx / FFP: CXR Post liver biopsy (SOB) one week earlier What are the possible causes of this lady’s dyspnoea?
Case 2. Dyspnoea & CXR white-out post transfusion • Fluid overload • Sepsis (infected blood) with ARDS • TRALI: transfusion-related lung injury • Donor Ab (esp HLA or neut) react with recipient WBC’s -> lung infiltrate • 1-6 hours post transfusion • Other features: fever, chills, low/normal CVP, BP, (neutropenia, monocytopenia) • Good prognosis for recovery if supported(e.g. ventilate) • Test donors: ?dangerous donor -> exclude.
Case 3. • A woman has just given birth • Suddenly she bleeds torrentially from the vagina and begins to ooze from mouth, nose and previous venepuncture sites • In terms of blood product support, What are your immediate actions?
Case 3. Post-partum haemorrhage(& generalised bleeding tendency) • PPH protocol – senior help, obstetric procedures/drugs etc • Blood samples: • FBC, PT/aPTT, Fibrinogen, D-Dimer • Crossmatch/order at least 4 units RBC(Consider use of O Neg flyers in LW fridge) • “Activate massive transfusion protocol (Obstetric)”: includes immediate release of2 units of FFP
Case 3. Post-partum haemorrhage(& generalised bleeding tendency) • Hb 7.4g/dL, WBC 15x109/L, plts 22x109/L • PT >60 secs (INR >12)aPTTR >12Fibrinogen 0.2g/L (n.r. 1.5-4.5)D-Dimer 25.4 mg/L FEU (n.r. <0.45) • Interpret these results.
Case 3. Post-partum haemorrhage(& generalised bleeding tendency) • Anaemia (bleeding) • Virtually unclottable blood • Low platelets • Consumption of all clotting factors • Very low Fibrinogen & high D-Dimer • Diagnosis:Disseminated Intravascular coagulation • What blood product(s) will you prescribe now?Where will you look for advice?
‘Policy for the transfusion of platelets, fresh frozen plasma and cryoprecipitate’
Case 3. D.I.C. • FFP 15ml/kg = 4 units for typical adult. Approx 1000mL – over 30-60mins • Platelets 1-2 ‘adult doses’ (1 unit = plts from 5 donations or one apheresis)Each unit over 15-20 mins • Cryoprecipitate 2 adult doses (1 unit = Cryo from 5 donations), when Fibrinogen <1g/L • RBC’s obviously needed. • Diagnose and treat underlying cause (e.g. amniotic fluid embolism, IUD)
Case 4. • A 25-year old man has acute leukaemia. He has received chemo, but is well with no bleeding other than mild petechiae on legs • Hb 10.5g/dL, WBC 0.4x109/L,Plts 15x109/L • What blood product(s) would you prescribe?Where will you look for advice?
Case 4. Acute Leukaemia, well.Hb 10.5g/dL, WBC 0.4x109/L, Plts 15x109/L • ‘Blood Products for Ward 34 patients’ • Platelet Transfusions: • For majority of patients give prophylactic platelets when Plt < 10 • For patients with additional risk factors aim to maintain Plt > 20 • Sepsis – when acutely septic • Concurrent use of antifungals (when acutely unwell) • Other abnormalities of coagulation (eg in those with APML) • Procedures (eg LP, line insertions, biopsies, urethral catheterisation, others) usually require Plt>50 • When a thrombocytopenic patient bleeds: 1 adult dose for mild bleed. • 2 adult doses for serious bleeding – and discuss with Consultant. • So does he need any platelets?