Download
1 / 11

E N D
Clinical features :-1- cough dry or productive2-Haemoptysis3-Chest pain4-Dyspnea5-Pleural effusion6-Anorexia & loss of weight7-Clubbing of the fingers8-Hoarseness of the voice (recurrent LN)9-Dysphagia involvement of the esophagus10-Hormonal syndromes ..ectopic ACTH , ADH, hypercalcaemia ,carcinoid syndrome Diagnosis Clinical , sputum cytology Chest X-ray ,CT chest .. Bronchoscopy ,BAL ,bronchial brush &biopsy FNAC….or Trucut biopsy , pleural fluid aspiration & cytology Diagnostic Thoracoscopy & mediastinoscopy TNM classification for staging
Signs of inoperability :-1-Bloody pleural effusion .positive for malignant cells2-Horner’s syndrome .3-Vocal cord paralysis4-Phrenic nerve palsy(elevated hemi diaphragm)5-SVC obstruction 6-Distant metastasis 7-If during surgery ,the tumor locally spreading or cannot be remover technically or fixed to the PA or to the heart ,it is technically irresectable
Treatment 1-Surgery more than 50%of the patients have distant metastases at the time of diagnosis .50% Iresectable per operatively15-20 % resectability rate Surgery ..segmentecomy , lobectomy . pneumectomy 2-Radiotherapy Pre operative or post operative Chemo therapy vincristine or adriamycin Bleomycin for malignant effusion
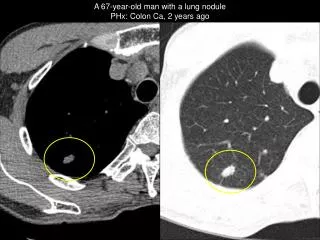
Differential diagnosis of a solitary lung lesion (COIN LESION) 1-Hydatid cyst 4- Primary benign lesion 2-Tuberculoma 5-primary malignancy of the lung 3-Angiomatous malformation (AV fistula) 6-metastatic tumors
Hydatid disease of the lung is caused by the .small. tape worm (EchinococcusGranulosus) Hydatid cyst means cyst full of water .It has a life cycle between dogs & sheep .Parasites in the elementary tract of the dog shed ova that excreted in the dog faeces , contaminated the food of the sheep in which hydatid cyst will develops in the viscera . Including the lung .Infected sheep when slaughtered and its entrails are eaten by dogs , the life cycle is completed .When a human being hands or food become contaminated with canine fecal material containing ova which will be ingested .The parasitic larva burrow through the gastric mucosa and are carried to the liver in the portal venous circulation where most of them filtered out to form hydatid cyst of the liver , some escape the liver & lodge in the lung to form one or more hydatid cyst which grows slowly or rapidly over years .
The cyst consists of a germinal layer & cyst fluid containing broad capsule & scoleses . A cellular white hyaline layers are laid down outside the cyst so that the cyst is enclosed by a laminated cyst membrane .As the cyst enlarged , it usually reaches the pleural surface . Compression of the lung tissues produces a thin fibrous layer of atelectatic lung tissue around the cyst (capsule , pericyst or adventia)
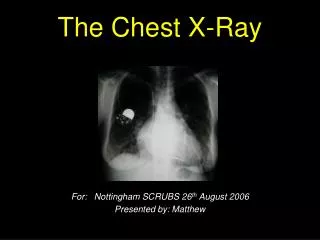
Clinical Manifestation • A-Asymptomatic • Any smooth homogenous opacity of uniform density with clear cut border and little or no reaction around it on a chest X-Ray is a hydatid cyst unless proved the other wise . • B-Cough & haemoptysis due to rupture of the cyst , or it can lead to severe dyspnea , or asphyxia ,or a hyper sensitivity reaction , • If the cyst get infected ,it will lead to formation of lung abscess or bronchiectatic changes .
Radiological Findings • 1-Smooth homogenous opacity (Intact H.C). • 2-Partial rupture (peri-vesicular pneumocyst). • 3-Complete rupture (Water –lilly sign) . • 4-Formation of lung abscess(Air –fluid level) . • 5-Completely coughed out cyst(empty cavity ) • 6-Rupture into the pleura (hydropneumothorax)
Treatment Surgical A-Inoculation means to remove it intact. B-Aspiration &evacuation technique C-Wedge resection or excision of the cyst with adjacent lung tissue. D-Segmentectomy ,Lobectomy or Pneumonectomy (rare ).