Download
1 / 49
490 likes | 618 Views
Learn about percutaneous ozone discolysis as a minimally invasive treatment for lumbar disc herniations. Explore epidemiology, mini-invasive techniques, pathogenesis of low back pain, disc-radicular conflict, and mechanisms of action of ozone therapy.

E N D
Percutaneous Treatment of LUMBAR disc herniations by ozone DISCOLYSIS AlperMuradov M.D. St.Sofia Hospital Sofia,Bulgaria
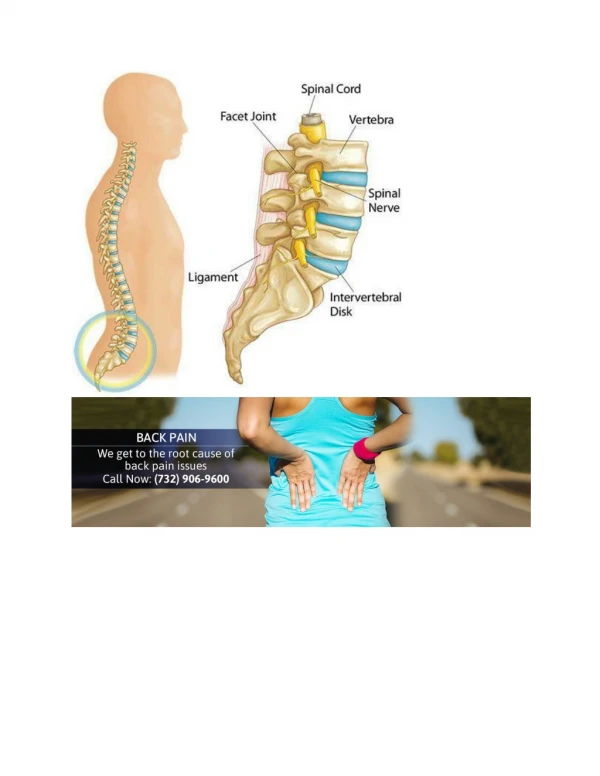
Epidemiology Low back pain is the commonest condition affecting the lumbar spine, and is the most frequent cause of absence from work. Around 80% of the population in western countries will experience at least one episode of low back pain in their lifetime and 55% suffer from low back pain associated with radicular syndromes.
Epidemiology In the United States alone around 200.000 patients with lumbalgia or sciatica are treated surgically every year. The short-term success rate after surgery for lumbosacral disc herniation is around 95-98% with a 2-6%, incidence of true recurrence of herniation. This percentage drops to around 80% in the long-term (more than 6 months) due to the onset of symptoms linked to Failed Back Surgery Syndrome (FBSS) characterised by recurrence and/or hypertrophic scarring with severe symptoms in 20% of patients and FBSS proper in 15%.
Mini Invasive Techniques These techniques have minimized the invasive nature of open surgery and avoid or decrease the complications associated with surgery. Reducing intervertebral disc size by mechanical aspiration of a part of the disc or partially dissolving the herniation by drying, reduces the conic pressure on the torn annulus and creates the space necessary for retropulsion whenever the circular fibres of the annulus regain a minimum capacity to contain the disc under tension. The strategy in these techniques is based on the fact, that a small change in volume produces large change in pressure.
Mini Invasive Techniques ASPIRATION LASER DISCECTOMY ENDOCOPY COBLATION CHEMONUCLEOLYSIS THERMAL COACULATION
Mini Invasive Techniques According to the site and the mechanism of action the MIS techniques can be divided in 3 groups: • DECOMPRESSIVE: • chemonucleolisys,percutaneous decompression and nucleodiscectomy, LASER and thermal discectomy • ANTIINFLAMATORY: Anti TNF therapy • COMBINED:Decompressive and direct antiinflamatory like coblationnucleoplasty and oxygen-ozone dicolysis
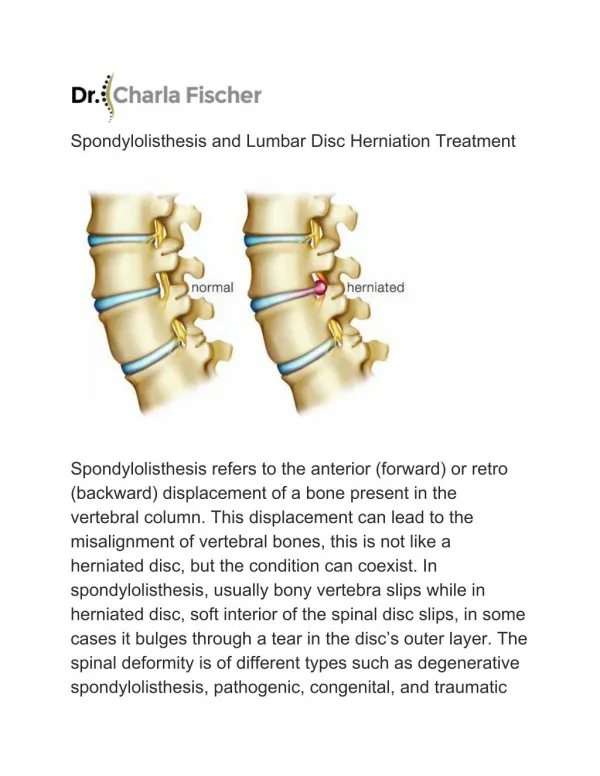
Pathogenesis of Low Back Pain Still discutable ,but 2 Main groups of factors are responsible: MECHANIC FACTORS DIRECT: -Direct pressure of hernia on the spinal ganglion -Deformation of the ligaments and anullus with stimulation of noccireceptors of Luschka’s nerve INDIRECT: -Ischemia due to compression on the arteries -Venous stasis INFLAMATORY FACTORS:The inflammatory factors are - cell-mediated response to the disc protrusion,possibly related to segregation of the disc to the immune system) - biohumoral factors like Phospholipase A2 (indirect inducer of pain mediators), Prostaglandin E2 (inflammatory inducer through Phospholipase A2), and Matrix metaloproteinases (MMPs)(inflammatory enhancers)
Pathogenesis Herniation of the nucleus pulposus is thought to trigger an autoimmune reaction, the proteoglycan component of its nucleus being segregated from the immune system after birth. Moreover the nucleus pulposus can also give rise to an inflammatory process through a non-immune-mediated mechanism supported by histiocytes, fibroblasts of the reactive perihernial tissue, and chondrocytes in the disc protrusions able to produce cytokines (Interleukin-1 alpha, Interleukin 6 and TNF-alpha). This lead to an increase in phospholipase A2 leading to the release of prostaglandin E2, leucotrenes and thromboxanes found in larger quantities in non-contained disc herniations and patients presenting more severe symptoms. Prostaglandins cause pain. In small amounts, they enhance sensitivity of the nerve roots and other pain-producing substances like bradykinin.
DISCO-RADICULAR CONFLICT COMPRESSION
DISCO-RADICULAR CONFLICT MECHANICAL COMPRESSION OF THE NERVE ROOT DOES NOT PROVOKE THE IRRADIATED PAIN
DISCO-RADICULAR CONFLICT compression edema obstacle to circulation Contracture of paravertebral muscles NEUROLOGICAL DISFUNCTION PAIN ischemia+pH
DISCO-RADICULAR CONFLICT Enzymes Phospholypase A2,prostaglandine E2 and Interleukine 6 are elevated in herniated disc and generate INFLAMATIONAND PAIN
DISCO-RADICULAR CONFLICT COMPARTMENT SYNDROME IIN THE NERVE ROOT AND IN THE GANGLION
DISCO-RADICULAR CONFLICT THIS LEADS TO EXTRINSIC COMPRESSION ON THE ROOT
DISCO-RADICULAR CONFLICT MECHANICAL INJURY OEDEMA VENOUS STASIS FIBRINOLITIC DEFICIT FIBROSIS
Mechanisms of Action of Ozone Mechanical: • Stimulates disruption of intra/inter – molecular valencies and leads to collapse of the 3D structure of proteoglycans and collagen of the disc. with features of nucleus pulposus matrix dehydratation and signs of regression (so called “disk mummification”).
Mechanisms of Action of Ozone Biochemical: • Strongly stimulating the local production of antioxidant enzymes • Intra- and trans-tissue oxygenation in the diseased site with reduced hypoxia and venous stasis. • Reduction of the cell-mediated process inhibiting proteinases release and an increase of the immunosupressor cytokines • Inhibition of inflammatory inducers (PPL) and pain-producing mediators ( ozone inhibits sinthesys of prostaglandines, liberation of bradikinines and other pain inducing products, secretion of proteinases from macrofages and polymorphous neutrophyles).
Mechanisms of Action of Ozone Direct: Some studies on histologic disc specimenns removed during open discectomy confirmed the direct effect of Ozone on the mucopolysaccharides making up the nucleus pulposus of the ruptured disc of water molecules and shrinkage of the disc,exerting compression on the nerve root.
Ozone Injection THROUH ALL THESE EFFECTS,OUR AIM IS TO OBTAIN -DISC DEHIDRATATION - NERVE METABOLISM CORRECTION - PAIN RELEIF
Technique • Lateral position • Posterolateralextraarticular • approach • Fluoroscopic C-arm system • Paralleling the vertebral plates • on AP and lateral proections
Technique -Chiba needles 20G -50 cc syringe -Sterile drapes
Procedure Paralleling The Needle
Procedure Puncture of the disc
Procedure Intradiscal infiltration (Ozone discography)
Procedure Epidural ozone diffusion
Procedure Intraforaminal injection of Local Anesthetic(Chirocaine, Dexametasone and Methylprednizolone
Procedure Sterile draping
Indications • -Low back pain and/or nerve root pain resistant to previous medical treatment, physiotherapy and other therapies at least 3 month -Paresthesia or hypoesthesia over the dermatome involved, mild muscle weakness and signs of root-ganglion irritation without motor loss. -CT and/or MR signs of small and medium-sized herniated discs correlating with the patient’s symptoms with or without degenerative disease complicated by intervertebral disc changes –protrusion or herniation -FBSS-residue of surgical discetomy with herniation recurrence and/or hypertrophic fibrous scarring
Contraindications: • Favism(G6PD deficiency) • Pregnancy • Disc herniation on CT/MRI corresponding to clinically severe motor deficit and/or sphincter disturbance • Free discal fragment • Severe spinal stenosis • Spinal instability • -Severe spondylosis with development of big osteophytes
Matherials and methods For the period 2008 - 2014 , 3049 patients underwent percutaneous injection of O2-O3 mixture for treatment of symptomatic disc herniations.All patients had CT/MRI,and complained of back pain and leg pain.The patients were divided in four groups: Group 1: L4-L5 or/and L5-S1 herniations Group 2: Multiple level herniated discs Group 3: Degenerative Disease complicated by herniation Group 4: Failed Back Surgery Syndrome(FBSS)
Results The results after procedure were evaluated by modified Mc Nab method,VAS and Oswestry Disability Index. Group 1 excellent 80,2% good 13,1% poor 6,7% ( 93,3) Group 2 excellent 75,6% good 15,5% poor 9,9%( 91,1) Group 3 excellent 49,1% good 22,7% poor 28,2%(71,8) Group 4 excellent 44,5% good 23,7% poor 31,8%(68,2)
Case 1 Before 4 months later
Case 2 Before 3 months later
Case 2 Before 3 months later
Case 3 Before 6 month later
Case 3 Before 6 month later
Case 4 Before 7 months later
Case 4 Before 7 months later
Complications • NO Cases Of adverse reactions • NO Cases Of spondylodiscitis • NO Cases Of root injury
Complications • Early-immediately after infiltration • Hypotension • Bradicardy0,4% • Collaps • Late • Fibrotisation over the site of infiltration 0,1%
Conclusion • Oxygen-ozone treatment of herniated disc is an effective and very safe procedure • Pain and functional results are similar to the outcomes for herniated discs treated with classic surgical discectomy • Complication rate is extremely lower (<0,1 %) • Recovery time is significantly shorter • No need for general anestesia • Do not modify normal spinal anatomy • Avoids bone demolition • Minimize peridural scarring
Conclusion • The O2-O3 intradiscal injection is: • SAFE • No lesions of intrevertebral disc and surrounding tissues • No periduralcicatrisation • No skin incision-lowered risk of infection • No muscle damage-no postoperative pain • No bone loss-no spinal instability • Do not except or impede open surgery if it is necessitated.