Download
1 / 46
540 likes | 938 Views
Imperial college. St Mary’s hospital. Charing Cross Hospital. Meniscal and Anterior Cruciate ligament injuries. Chinmay Gupté PhD (Dip IC), FRCS (Tr&Orth), MA (Oxon), BMBCh Consultant Orthopaedic Surgeon/Senior Lecturer E Ali, Trauma Fellow A Dodds, SpR

E N D
Imperial college St Mary’s hospital Charing Cross Hospital Meniscal and Anterior Cruciate ligament injuries Chinmay Gupté PhD (Dip IC), FRCS (Tr&Orth), MA (Oxon), BMBCh Consultant Orthopaedic Surgeon/Senior Lecturer E Ali, Trauma Fellow A Dodds, SpR Imperial College Hospitals and Imperial College London
Competing interests • none
What’s our agenda? • Improve our practice • Enhance our knowledge • Address controversies • Cutting edge technologies/treatments
Summary • Anatomy • Biomechanics • Meniscal tears: repair or resect? • Meniscal deficiency • ACL: what’s new? • (PCL) • Emerging technologies
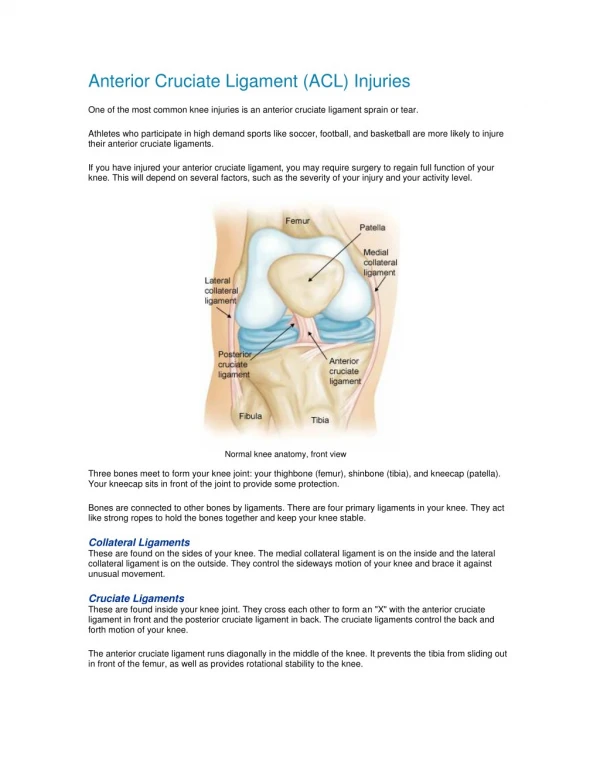
Medial Lateral Anterior Menisci anatomy • Menisci • Intraarticular knee structures • Semi-lunar (axial) • Wedge-shaped (coronal/saggital) • Fibro-cartilaginous (type I Collagen) Lateral Medial Anterior
pMFL Femur PCL LM dMCL MFLs aMFL Medial InsertionalLigaments Lateral Anterior Tibia AIL Meniscal attachments • Meniscal ligaments • Insertional • Anterior Intermensical (AIL) • Mensicofemoral (MFLs) • Deep Medial Collateral (dMCL)
Histology and biomechanics • Histology1-3 • Tissue bulk: circumferentialfibre bundles (Type I) • Surface:Meshwork of thin fibrils/radial tie fibres (Taken from: Petersen & Tillmann, 1998, Anat Embryol) 1Petersen & Tillmann 1998, AnatEmbryol 2Bullough et al. 1970, JBJS-Br 3Beaupre et al. 1986, CORR 4Tissakht & Ahmed 1995, J Biomech
Meniscus functions • Reduce contact stresses • Load spreaders • Shock absorbers • Stability • Lubrication • Proprioception • Nutrition
Femur Tibia Load transmission • Axial load transferred through the joint is converted into meniscal hoop stresses • The meniscus • conforms to thefemoral condyles • increases its circumference • translates outwards • spreads the load overa large contact area • hence reduces the stresses on the underlying cartilage 70-99% of the joint load is carried by the menisci1 • Insertional ligaments are key 1Seedhom & Hargreaves, 1979, Eng Med
Lateral Medial Anterior Insertional ligaments • Anchor menisci on tibial plateau • Control meniscal motion • Prevent excessive meniscal extrusion • Loss of one completely de-functions the meniscus • Tensile modulus in human1 ~ 90 MPa ~ 75 MPa ~ 90 MPa ~ 165 MPa 1Haut-Donahue & Hauch, July 2008, ESB
Meniscal “ligaments” stabilise knee 1Gupte et al, 2003, Arthroscopy 2Gupte et al, 2003, JBJS-Br 3Amadi et al, 2008, KSSTA 4Gupte et al, 2002, J.Biomech. 5Kohn & Moreno, 1995, Arthroscopy 6Nelson & LaPrade, 2000, AJSM 7Berlet & Fowler, 1998, AJSM 8Robinson et al, 2006, AJSM
Intact Meniscectomised Total meniscetomy • Meniscectomy results in1-3 • Cartilage to cartilage contact • Less conformity • Decreased contact area • Increased contact stresses(up to 200%)1 • Increased shear stresses 1Baratz et al, 1986, AJSM2Seedhom & Hargreaves, 1979, Eng Med3McDermott et al, 2008 KSSTA (Taken from: McDermott et al, 2008 KSSTA)
Meniscetomy Stresses Removal of meniscus: reduce surface area of contact>>>increased contact stresses Does repair restore meniscal stress function??? No long term studies
Meniscectomy consequences Lateral meniscectomy results in OA; also probably medial Late degenerative changes after meniscectomy. Factors affecting the knee after operation.PR Allen, RA Denham, and AV Swan.JBJS1984 Chatain 2001 KSSTA Brophy RH, Gill CS, Lyman S, et al. Effect of anterior cruciate ligament reconstruction and meniscectomy on length of career in National Football League athletes: A case control study. Am J Sports Med 2009;37:2102-2107.
Meniscal Tears • Circumferential • parallel to the load-bearing fibres • small effect on meniscal function • Radial – Vertical • cut across the load-bearing fibres • large effect on meniscal function • Flap • Bucket handle • Horizontal cleavage • Complex Circumferential Radial Axial Radial Tear
Meniscal Tears: treatment options • Conservative • Repair • Partial meniscectomy • Total meniscectomy • Allograft transplantation • Implants (?) • Tissue engineering (?) (Taken from: Arnoczky & Warren, 1983, AJSM)
Meniscal Tears: “let’s repair them all”But: • Complex tear repairs have poor outcomes • Repair vs reconstruction results not clear cut (Shelbourne) • Complications of repair: • Chondral scuffing (Anderson) • Hardware loose/Dart indentation • Failed repairs lead to more meniscal loss • Persistent pain • Nerve damage Shelbourne, K.D. and D.R. Carr, Am J Sports Med, 2003. 31(5): p. 718-23. Meniscal repair compared with meniscectomy for bucket-handle medial meniscal tears in anterior cruciate ligament-reconstructed knees. Anderson Arthroscopy 2000; Austin AJSM 1993
Meniscal Repair Versus Partial Meniscectomy: A Systematic Review Comparing Reoperation Rates and Clinical Outcomes. Paxton et al Arthroscopy 2011 Lower reoperation rate with repair after ACLR “Whereas the combined reoperation rate after a partial meniscectomy is quite low, at 4%, the relatively high reoperation rate of almost 23% after meniscal repair may be acceptable if there is a potential long-term benefit to the joint. The lower reoperation rate of 14% after meniscus repair at the time of ACLR is even more likely to be acceptable assuming long-term benefit can be shown.”
Repair Technique • Inside out is Gold standard: • Large bucket handle especially posterior portion • Double barrelled guide • Stryker retraction tool • 2’0 suture eg ethibond • Anterior to gastroc • Watch saphenous nerve medially and peroneal laterally
Technique • All inside (Ultra fastfix): • Better newer prostheses • Portals slightly higher • 1.4mm on stop • Avoid scuffing • Vertical sutures: radial tie fibres • Curved needles • 2up/1down
Controversies • White/white zone tear: younger/longitudinal/lateral/ACLR • Rasping/trephining:stable/<1cm/partial tear • Post op regime: NWB (Taken from: Arnoczky & Warren, 1983, AJSM) Trephining: Zhongman et a arthroscopy 1996;White on white: Gallagher et al knee 2010 and Noyes AJSM 2002
Meniscal replacement- artificial • Products exists • Require • Stable rim of meniscal tissue • suture • ?normal mechanics • Menaflex: FDA approval withdrawn 2010
Meniscal transplant • Normal articular cartilage • Technically demanding • Fixation issues:either suture to capsule OR bone plugs • Sizing issues • ?normal mechanics • ?reduced degenerative change Marcacci et al AJSM 2012Verdonk et al JBJS A 2005 and 2006
Imperial Meniscus Patent filed Polyurethane Unique structure Wear testing Animal studies Fixation testing
ACL established knowledge • Resists anterior drawer/pivot shift • Double bundled functionally • ACL rupture >>> medial meniscal tears • ACL reconstruction reduces MM tear (Meunier Acta O Scand 1999) • Mensical repair more successful with ACLR
ACL controversies • Tunnel positions • Does ACLR obliterate Pivot shift? • Single vs double bundled • Extra articular reconstruction
Natural history of the unstable ACL deficient The ACL Injury Cascade ACL disruption Subluxation Giving way Meniscal injury Sports disability Joint arthrosis
ACL bundles • AM bundle: tight in flexion (anterior drawer) • PL bundle tight in extension (Lachmanns) • PL bundle: further away for axis of rotation (resists pivot)
ACL Tunnel position: femur Harner JBJS A 2000
ACL Tunnel positions • Femoral tunnel has become more oblique with time (more anatomic) • Has this led to increased rerupture rate?
Non anatomic Tunnel positions Anatomic Non anatomic
Tunnel position • Ensure adequate notch clearance: vertical PCL • Drill through medial portal (?view accessory medial portal) • 10:00 (R) or 2:00 (L) position • Mark with chondral pick 70degrees • ?use offset guide/guide wire • 4.5mm solid drill • Ensure knee fully flexed • Tibia: 2/3rds along line from anterior horn LM insertion to medial tibial spine
Single vs double bundled Double bundled More anatomic Greater control of pivot (93% vs 67% Hussein et al) Better tunnel position Single bundled: DB technically challenging No better functional results with DB More oblique SB just as good Differential failure of DB bundles Adachi et al JBJS 2004 RCT Single vs double no difference Meredick metaanalysis AJSM 2008 no difference Yasuda Arthroscopy 2006 better but n=4 Siebold Arthroscopy 2008: RCT DB better results Hussein ..&Fu AJSM 2011 RCT 5 yr results DB better pivot but no functional difference
Pivot • Main functional problem in ACL rupture is the pivot phenomenon • SB reconstruction does not obliterate pivot in 33% (Hussein 2011) • Double bundled: Greater control of pivot (93%, Hussein) • But more technically difficult/no functional benefit • Is there any other way to deal with the pivot? • Extraarticular augmentation of ACL reconstruction Galway HR, Beaupre A, MacIntosh DL. Pivot shift: a clinical sign of symptomatic anterior cruciate insufficiency. J Bone Joint Surg. Br 1972;54:763-4. Zantop et al Arch Orth Trauma Surg 2010
Previous extra-articular reconstruction • Used as an isolated technique and combined with intra-articular techniques. • First description by Hey- Groves- 1920 • Several different methods popular: • Lemaire • MacIntosh • Ellison • Losee • Marcacci
MacIntosh reconstruction Used strip of ITB- the ‘lateral substitution’ reconstruction
Marcacci Repair Hamstring graft as intra-articular reconstruction with extra-articular augmentation
Extra articular reconstruction: poor historical results • Failure of isolated extraarticular reconstruction and recurrent instability (Dandy 1995) • Degenerative change in the lateral compartment (Roth 1987; Strum 1989) • But… • Stretch of tenodesis in isolated extraarticular or augmented with nonanatomic intraarticular placement • Degenerative change from 4 weeks in plaster post op • Newer rehab techniques and braces Neyret et al: Extraarticular tenodesis in skiiers BJSM 1994
Can we do any better? • Understand anterolateral capsular anatomy (Segond fracture) • Assess new procedures biomechanically in vitro • A more ‘anatomic’ approach may prevent some of the problems from the past:- • Reduce failure rates • Decrease risk of lateral ‘overtightening’ • Minimally invasive techniques to avoid large scars
Other issues in ACL • Hamstrings vs BTB (Aglietti et al /Pinczewski et al) • Rehab: open vs closed chain • Multiligament
Conclusions Sir William Osler (1849-1919) • Anatomy and basic biomechanics is key • Manage the patient not the book/paper "He who studies medicine without books sails an uncharted sea, but he who studies medicine without patients does not go to sea at all." "Listen to your patient, he is telling you the diagnosis,"