Download
1 / 53
560 likes | 916 Views
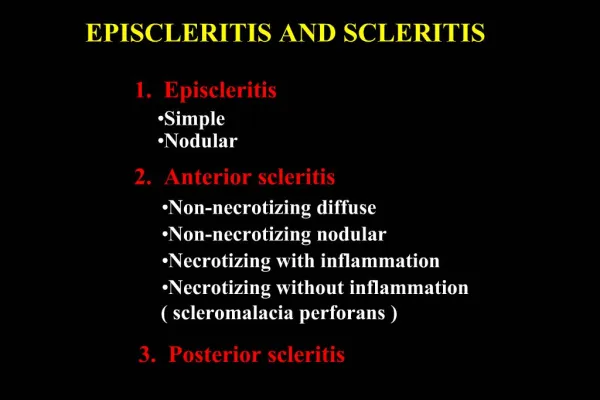
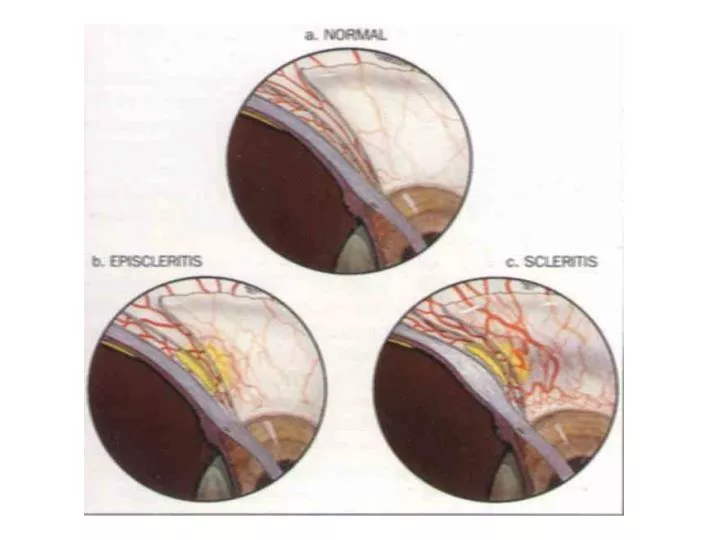
EPISCLERITIS is a benign, self limiting and recurrent disorder of the episcleral tissue, affects both sexes,especially young adults, the onset is sudden with intense redness involving only one quadrant of the globe + mild discomfort

E N D
EPISCLERITIS is a benign, self limiting and recurrent disorder of the episcleral tissue, affects both sexes,especially young adults, the onset is sudden with intense redness involving only one quadrant of the globe + mild discomfort the affected episclera is edematous, the blood vessels is engorged (simple scleritis) nodular episcleritis is characterized by a nodule surrounding injection; the condition tends to spontaneous remission with marked tendency for recurrence Treatment: topical steroids and/or non-steroidal antiinflamatory drugs, in severe forms – sistemic flurbiprofen (100mg three times daily) or indomethacin (75mg/day) are indicated.
SCLERITIS is a granulomatous inflamation involving the colagenous coat of the eye.There is 5 types of scleritis: diffuse anterior scleritis (the most common and most benign type) – diffuse engorgement of episcleral and scleral vessels, resulting a violaceous hue. 25% of pacients have an identifiable systemic disease (rheumatoid arthritis) nodular anterior sceleritis – is characterized by single or multiple nodules beneath the episcleral tissue ( tender and immobile); it may be associated with collagen vascular disease; necrotizing anterior scleritis – with marked inflamation + severe pain + intense inflamatory reaction. Complications is made by scleral thining and 40% have a decrease in visual acuity (association with systemic autoimmune disease);
necrotizing anterior scleritis – with minimal inflamation(sleromalacia perforans) inflamation and pain are minimal; progresive scleral thining occurs, sometime resulting in bulging staphylomas; it is most commonly seen in patients with long-standing rheumatoid arthritis; posterior scleritis – pain, redness and decrease in V.A.; proptosis, ptosis + lid edema; funduscopicfindings may include serous retinal detachement, choroidal folds, disc edema . Treatment: oral nonsteroidal antiinflammatory drugs (flurbiprofen, indomethacin) oral prednison (40-80 mg daily, in patients who are resistent to or intolerant of NSAID combination of an NSAID and lower dose of steroid topical steroids (reducing pain and redness) immunosupresive drugs(cyclophosphamide, azathioprine, cyclosporine) in steroid rezistent cases.
UVEITIS • Uveitis is a major cause of visual impairment and may account for 10-15% of blindness in the USA. • Of people aged under 65 who are registered legally blind, 10%are visually compromised because of uveitis and its complications, verynearly the same number affected by diabetic retinopathy
Uveitisanatomical classification • Anterior uveitis • Iritis • Iridocyclitis • Intermediate uveitis • Posterior uveitis • Panuveitis
Anterior uveitis • HLA-B27 Positive or Seronegative Group • Ankylosingspondylitis • Reiter’s syndrome • Inflammatory bowel disease (Ulcerative colitis, Crohn’s disease) • Psoriatic arthritis • Intraocular lens related • Herpes simplex • Herpes zoster • Trauma • Juvenile rheumatoid arthritis • Fuchs’ Heterochromiciridocyclitis • Behcet’s disease • Sarcoidosis • Tuberculosis • Syphilis • Glaucomatocyclitic crisis • Lens-induced uveitis • Idiopathic
ANTERIOR UVEITIS Is the inflamation of the iris and ciliary body = iridociclitis Clasification : exogenous and endogenous, acute and chronic. Diagnosis : red eye (ciliary injection) with precipitates on cornea, or hypopian in anterior chamber. The pupil is in miosis and after atropine 2% is irregular because there are posterior synechias between iris and lens. Intraocular pressure is normal or decreased. It must be differentiated by keratitis, conjunctivitis and angle closure glaucome (acute) Treatment: corticosterois local and sistemic and in severe forms immunosupressive. Atropine , antibiuotis or antivirals
Symptoms : • decrease vision • lacrimation • photophobia • redness • Signs: • ciliary injection • keratic precipitates • aqueous cells • aqueous flare • posterior synechia
complications • Posterior synechiae • Cataract • Glaucoma • Macular oedema • Cyclitic membrane • Phtisis bubi
Treatment • Steroids • Cycloplegics • Mydriatics • Immunosuppressives: • Antimetabolites (azathioprine, methotrexate) • T-cell inhibitors (cyclosporin, tacrolimus) • Cytotoxic agents (cyclophosphamide, chlorambucil)
PARS PLANITIS • Is chronic cyclitis, or intermediative uveitis. • Is a common inflamatory disease of inferior portion of the ora serrata. Is often bilateral of children and young adults • Diagnosis: vitrous exudate = snowballs, viaion acuity is decreased and exudate on the pars planitis (snowbanking). • Treatment : subtenon injection of a long-acting corticoid or oral steroids. • Other therapy: cryotherapy, cyclosporine or cyclopentholate
Pars planitis(intermediate uveitis) • Pars plana involvement; sometimes retina and coroida till the ora serata • Simptoms: • floaters • VA decrease (MCE, vitrious floaters) • Signs: • Vititis
Complications: • MCE, • Cataract • RD
POSTERIOR UVEITIS: It is the inflamations of the choroid and retina = chorioretinitis. Diagnosis: Vitreous opacities – clouding the vitreous body and visual acuity is decreased (is an exudate). Ophthalmoscopically appears as black spots in red background. Choroiditis – acute – ill-defined grayish yellow or grayish white area surrounded by normal colored fundus. In chronic form the areas appears with pigmented surrounded.Causes: tuberculosis, sarcoidosis, toxoplasmosis. Treatment – for causes and corticosteroids. TOXOPLASMOSIS: Is caused by intracellular protozoa – Toxoplasma gondii (the cat is the definitive host). Clasification : congenital and aquired. Congenital toxoplasmosis: occurs in utero during the first 7 months of pregnancy. Than appears fever, lymphadenopathy, chorioretinitis Chorioretinitis – fovea is destroyed, causing loss of central vision.The lesion is with atrophy and pigmented borders. Aquired posterior uveitis with inflamation of the choroid and retina with vitreous exudates. Treatment –trisulfapyrimidine or clindamicin. corticosteroids.
Posterior uveitis • Infection • Toxoplasma • Histoplasmosis • Cytomegalovirus • Toxocara • Herpes simplex • Syphilis • Tuberculosis • Candida • Retinal vasculitis • Sarcoidosis • Sympathetic ophthalmia • Behcet’s disease • Idiopathic
posterior uveitis refers to inflammation involving the retina, choroid or optic nerve
Occlusive retinal vasculitis in a patient with Behçet’s disease. There is also an epiretinal membrane temporal to the fovea, and moderate optic disc pallor
Sympathetic ophthalmia • Sympathetic ophthalmia is inflammation of the uveal tract after trauma or surgery to the other eye • granulomatous uveitis that occurs after penetrating trauma or surgery to the other eye • underlying mechanism is thought to be an autoimmune reaction directed against melanin-containing cells in the uvea
SYMPATHETIC OPHTHALMIA • Is a bilateral, diffuse, granulomatous inflamation of the uvea. It appears afeter days or years after a trauma (penetrating) or after surgery for cataracts or glaucoma. • It is possible because the hypersensitivity type IV. T • The injured eye (exciting eye) has a torpid, persistent uveitis and after that it appers an uveitis to the fellow eye (sympathizing eye). Vision acuity is very decreased, the eyes are red with ciliary injection and exudate in anterior chamber. • Treatment: enucleation of the exciting eye, cyclosporine, corticosteroids.