Download
1 / 25

E N D
Please note, these are the actual video-recorded proceedings from the live CME event and may include the use of trade names and other raw, unedited content. Select slides from the original presentation are omitted where Research To Practice was unable to obtain permission from the publication source and/or author. Links to view the actual reference materials have been provided for your use in place of any omitted slides.
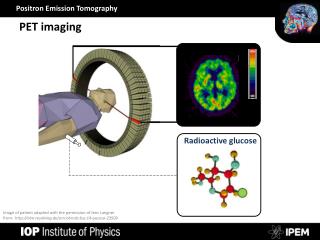
Multi-Modality Management of Stage III NSCLC Use of PET Imaging Walter J Curran, Jr, MD Executive Director Winship Cancer Institute of Emory University Georgia Cancer Coalition Distinguished Scholar RTOG Group Chair
Good PS Stage III NSCLC: Where is There No Randomized Data? • Use of Any Advanced Technology RT Tools? • Selection of Best Chemo to Give Concurrently with RT • Use of Functional Imaging in RT Planning/Assessment • Higher RT Dose with a Standardized Chemo Regimen • Use of “Targeted Agent” Concurrent with Chemo-RT
State III NSCLCSurvival by Local Tumor Control Status • Median Survival • Pts with Local Control (n=674) • 18.6 mo • 24% • Pts without Local Control (n=761) • 15.5 mo • 6% • p < 0.0001
RTOG 0617 (CALGB 30609, NCCTG N0628)Randomized Phase III Trial of Standard-Dose (60 Gy) Versus High-Dose (74 Gy) Conformal RT w Concurrent and Consolidation Cb/P in Stage IIIA/B NSCLC Concurrent ChemoRT Paclitaxel 45 mg/m2 Carboplatin AUC 2 Weekly x7 RT 60 Gy (2 Gy/d) + Cetuximab RANDOM I ZE Stage IIIA/B PS 0-1 FEV1 ≥1.5L; V20 <37% No Supraclav LNs PET recommended Consolidation Paclitaxel 200mg/m2 Carboplatin AUC 6 q3wks x2 cycles Concurrent ChemoRT Paclitaxel 45 mg/m2 Carboplatin AUC 2 Weekly x7 RT 74 Gy (2 Gy/d) + Cetuximab Primary Endpoint – Survival (n=512) (2 X 2 design evaluating dose and cetuximab independently) Stratified by stage (A vs B), type of RT (3-D vs IMRT) and PS (0 vs 1)
RTOG 0617 DMC Meeting June 2011 • DMC Meeting in early June 2011 • High Dose RT Arm (74 Gy) Crossed Futility Boundary • Both 74 Gy Arms Closed to Further Accrual • Cetuximab Question at 60 Gy to be Completed • Accrual will Finish in Late 2011/Early 2012
RTOG 0617: Standard vs High RT Dose Question • 423 Patients Evaluated in June 2011 DMC Analysis • Median Follow-up is 9 months • After 90 Deaths, High RT Dose Arm Crossed Futility Boundary • 10 Treatment-Related Deaths: • 3 in Standard Dose Arm • 7 in High Dose Arm • Most other Deaths Attributed to Disease Progression
RTOG 0617 Overall Survival • 60 Gy, 58 deaths/213 • 74 Gy, 70 deaths/204 • HR=1.45 (1.02, 2.05) • p=0.02* • *One-sided p-value, left tail
Can PET/CT Assess RT or ChemoRT Efficacy Earlier?This may be the Most Personalized Care for Stage III Patients!
FDG-PET-based Response as an Early Marker of Survival (Hicks J Nuc. Med 2009)
ACRIN 6668/RTOG 0235 Use of PET in Response Assessment FDG - P ET - SUV R E G I S T E R FDG - PET – SUV to be done 12 to 16 weeks following XRT and several wks after adjuvant chemo (if given). Concurrent chemo-XRT (+/- adjuvant chemo as per M.D.) Sample size = 250 pts. Completed Accrual 5/14/09 P.I.: Machtay
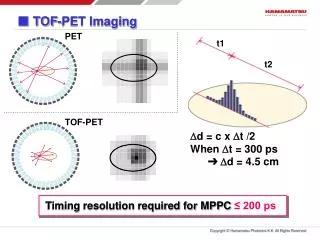
SUVpeak (c.f. SUVmax) SUVpeak: Circular 1 cm ROI centered around SUVmax. Then, the software is queried to determine the mean SUV within that precisely defined ROI.
RTOG 0235/ACRIN 6668Pre and Post- Chemo-RT SUV Median SUV= 2.5 Median SUV= 9.4
Major Limitation . . . 12-16 week waiting period following RT before assessing response/efficacy/prognosis/prediction can seem like an eternity!
PET during Weeks 1&2 of RT "The location of the low and high FDG uptake areas within the tumor remained stable during RT. This knowledge may enable selective boosting of high FDG uptake areas within the tumor." Aerts HJWL, IJROBP 2008
Mid-course FDG-PET & Outcome "Although there were not enough patients to perform survival analyses in this study, a significant association of metabolic response and peak FDG activity between during-RT and post-RT scans suggests a potential of using the during-RT PET response (at approximately 45 Gy) to predict long-term survival in lung cancer." Kong, JCO 2007
PET-based Adaptive Radiotherapyfor Stage III NSCLC – RTOG 1106 Off Study – D/C RT PD R E G I S T E R ChemoRT 44 Gy FDG-PET FDG-PET RT to 64 Gy. R A N D O M I Z E SD/Response RT to 64 Gy + 10+ Gy boost based on FDG-PET
FDG-PET based Adaptive RT "Tumor metabolic activity and volume can change significantly after 40-50 Gy of RT. Using mid-RT PET volumes, tumor dose can be significantly escalated or normal tissue complication probability reduced." Feng, IJROBP 2009
Lung Functional Region Classification CT and Ventilation-SPECT • Lung quality and ventilation-SPECT is variable between lungs • Radiation planning identifying partially functioning, dysfunctional and functional lung can assist in individualizing therapy
V/Q SPECT to Individualize Adaptive RT The dose of a functioning lung region decreases from 30-50% to 15-30% after re-optimization.
Summary: Stage III NSCLC Chemo-RT • No Fully Personalized Therapy • Thoracic RT is Becoming Anatomy and Response Dependent • RT Optimization of Interest Despite RTOG 0617 • Changes in Details of Care not All Subject to Clinical Trials
Sunday, February 12, 2012Hollywood, Florida Co-Chairs Rogerio C Lilenbaum, MD Mark A Socinski, MD Co-Chair and Moderator Neil Love, MD Faculty Walter J Curran Jr, MD David Jablons, MD Mark G Kris, MD Suresh Ramalingam, MD Alan B Sandler, MD