Download
1 / 1
10 likes | 106 Views
Effects of Hypercapnic Hyperpnoea during Emergence on PACU Recovery Dwayne Westenskow PhD, Noah Syroid M.S, Diane Tyler R.N, Julia White R.N, Frederike Bruehschwein M.S, Cameron Jacobson B.S, Sarah Beaty B.A, Laurel Kay R.N, Joseph Orr PhD, Derek Sakata M.D.

E N D
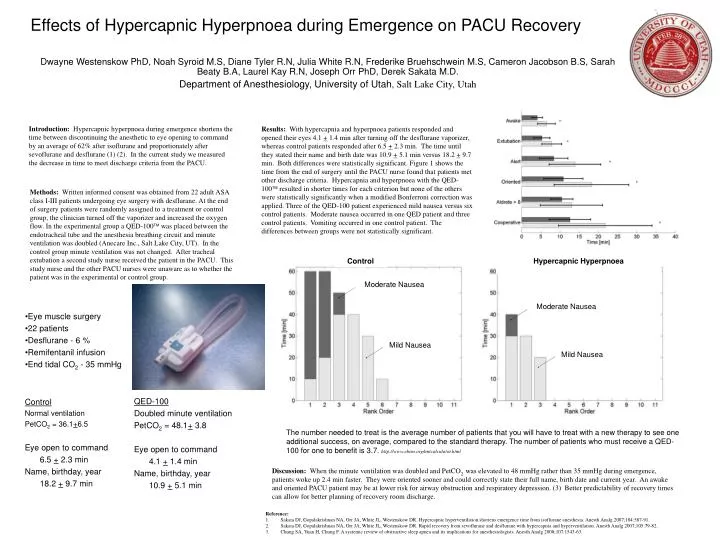
Effects of Hypercapnic Hyperpnoea during Emergence on PACU Recovery Dwayne Westenskow PhD, Noah Syroid M.S, Diane Tyler R.N, Julia White R.N, Frederike Bruehschwein M.S, Cameron Jacobson B.S, Sarah Beaty B.A, Laurel Kay R.N, Joseph Orr PhD, Derek Sakata M.D. Department of Anesthesiology, University of Utah, Salt Lake City, Utah Introduction: Hypercapnic hyperpnoea during emergence shortens the time between discontinuing the anesthetic to eye opening to command by an average of 62% after isoflurane and proportionately after sevoflurane and desflurane (1) (2). In the current study we measured the decrease in time to meet discharge criteria from the PACU. Results: With hypercapnia and hyperpnoea patients responded and opened their eyes 4.1 + 1.4 min after turning off the desflurane vaporizer, whereas control patients responded after 6.5 + 2.3 min. The time until they stated their name and birth date was 10.9 + 5.1 min versus 18.2 + 9.7 min. Both differences were statistically significant. Figure 1 shows the time from the end of surgery until the PACU nurse found that patients met other discharge criteria. Hypercapnia and hyperpnoea with the QED-100ä resulted in shorter times for each criterion but none of the others were statistically significantly when a modified Bonferroni correction was applied. Three of the QED-100 patient experienced mild nausea versus six control patients. Moderate nausea occurred in one QED patient and three control patients. Vomiting occurred in one control patient. The differences between groups were not statistically significant. Methods: Written informed consent was obtained from 22 adult ASA class I-III patients undergoing eye surgery with desflurane. At the end of surgery patients were randomly assigned to a treatment or control group, the clinician turned off the vaporizer and increased the oxygen flow. In the experimental group a QED-100ä was placed between the endotracheal tube and the anesthesia breathing circuit and minute ventilation was doubled (Anecare Inc., Salt Lake City, UT). In the control group minute ventilation was not changed. After tracheal extubation a second study nurse received the patient in the PACU. This study nurse and the other PACU nurses were unaware as to whether the patient was in the experimental or control group. Control Hypercapnic Hyperpnoea Moderate Nausea Moderate Nausea • Eye muscle surgery • 22 patients • Desflurane - 6 % • Remifentanil infusion • End tidal CO2 - 35 mmHg Mild Nausea Mild Nausea QED-100 Doubled minute ventilation PetCO2 = 48.1+ 3.8 Eye open to command 4.1 + 1.4 min Name, birthday, year 10.9 + 5.1 min Control Normal ventilation PetCO2 = 36.1+6.5 Eye open to command 6.5 + 2.3 min Name, birthday, year 18.2 + 9.7 min The number needed to treat is the average number of patients that you will have to treat with a new therapy to see one additional success, on average, compared to the standard therapy. The number of patients who must receive a QED-100 for one to benefit is 3.7. http://www.ebem.org/nntcalculator.html Discussion: When the minute ventilation was doubled and PetCO2 was elevated to 48 mmHg rather than 35 mmHg during emergence, patients woke up 2.4 min faster. They were oriented sooner and could correctly state their full name, birth date and current year. An awake and oriented PACU patient may be at lower risk for airway obstruction and respiratory depression. (3) Better predictability of recovery times can allow for better planning of recovery room discharge. Reference:1. Sakata DJ, Gopalakrishnan NA, Orr JA, White JL, Westenskow DR. Hypercapnic hyperventilation shortens emergence time from isoflurane anesthesia. Anesth Analg 2007;104:587-91. 2. Sakata DJ, Gopalakrishnan NA, Orr JA, White JL, Westenskow DR. Rapid recovery from sevoflurane and desflurane with hypercapnia and hyperventilation. Anesth Analg 2007;105:79-82. 3. Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg 2008;107:1543-63.