Download
1 / 3
30 likes | 138 Views
Case of the week 08-23: A tricky diagnostic challenge: (page 1 of 3).

E N D
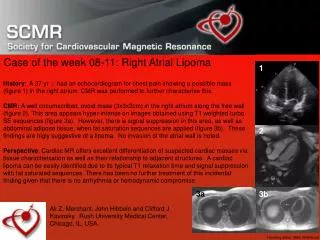
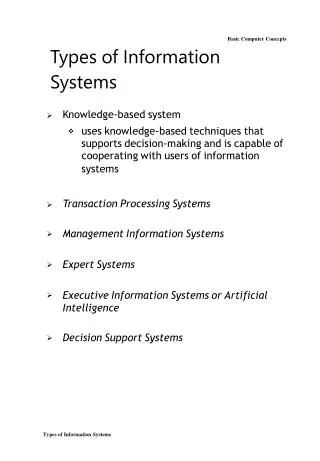
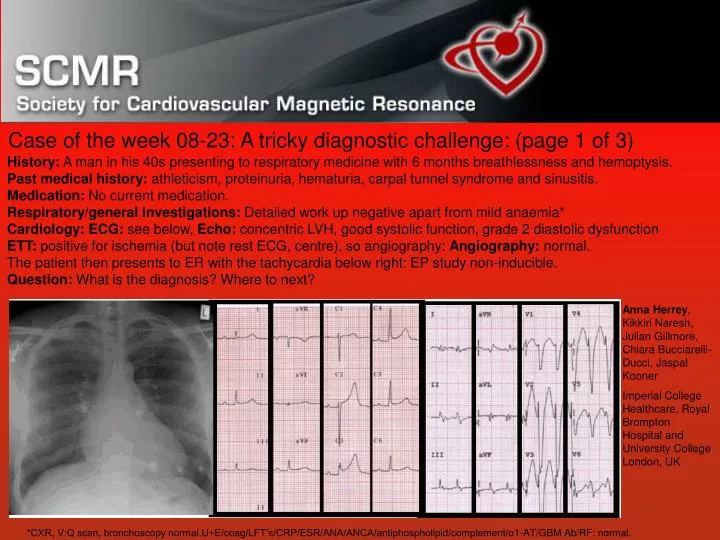
Case of the week 08-23: A tricky diagnostic challenge: (page 1 of 3) History: A man in his 40s presenting to respiratory medicine with 6 months breathlessness and hemoptysis. Past medical history: athleticism, proteinuria, hematuria, carpal tunnel syndrome and sinusitis. Medication: No current medication. Respiratory/general investigations: Detailed work up negative apart from mild anaemia* Cardiology:ECG: see below, Echo: concentric LVH, good systolic function, grade 2 diastolic dysfunctionETT: positive for ischemia (but note rest ECG, centre), so angiography: Angiography: normal.The patient then presents to ER with the tachycardia below right: EP study non-inducible. Question: What is the diagnosis? Where to next? Anna Herrey, Kikkiri Naresh, Julian Gillmore, Chiara Bucciarelli-Ducci, Jaspal Kooner Imperial College Healthcare, Royal Brompton Hospital and University College London, UK *CXR, V:Q scan, bronchoscopy normal.U+E/coag/LFT’s/CRP/ESR/ANA/ANCA/antiphospholipid/complement/α1-AT/GBM Ab/RF: normal.
Case of the week 08-23: A tricky diagnostic challenge (page 2 of 3) Cine CMR: Marked biventricular long axis reduction with preserved radial function. Mild concentric LVH. Contrast CMR: Remarkable, extensive LGE in a non-ischemic pattern, most prominent subendocardiallyCMR diagnosis: Likely cardiac amyloidosis
Case of the week 08-23: A tricky diagnostic challenge (page 3 of 3) Subsequent investigation: Cardiac biopsy (right) showed green birefringence on Congo red staining confirming cardiac amyloid (note thickened arteriolar wall). A bone marrow biopsy showed plasma cells (left) and Lambda light chains (middle), and urine showed excessive lambda light chains. Management and follow-up: ‘light’ chemotherapy (prednisolone /melphalan). Serial echo demonstrated progression to restrictive physiology and systolic dysfunction. Work-up for cardiac transplant commenced with a plan for intensive chemo & stem cell transplant, but events overtook this plan with end stage renal and cardiac failure. Conclusion: CMR frequently solves the most complex diagnostic conundrums, here cardiac amyloidosis, although in this case, the outcome was poor.