Download
1 / 1
10 likes | 227 Views
Clinical History : 2 day old ♀, mild respiratory distress. Clinical examination : Holosystolic murmur at the mid-sternal border. CXR : Esophageal atresia with tracheoesophageal fistula.

E N D
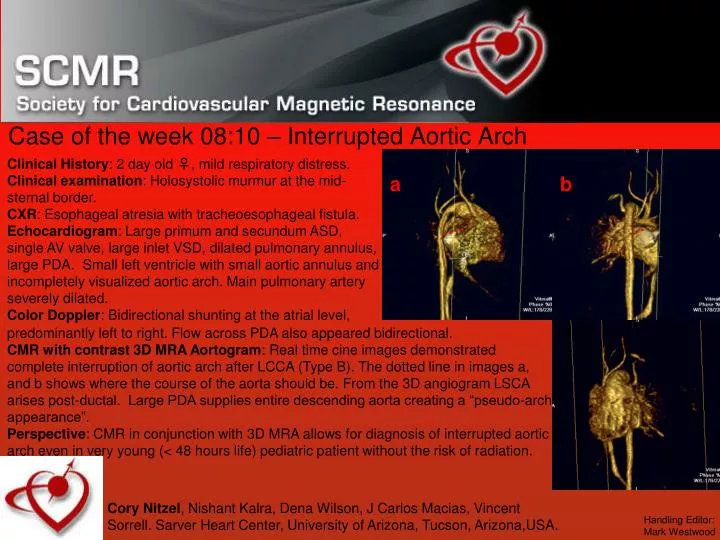
Clinical History: 2 day old ♀, mild respiratory distress. Clinical examination: Holosystolic murmur at the mid-sternal border. CXR: Esophageal atresia with tracheoesophageal fistula. Echocardiogram: Large primum and secundum ASD, single AV valve, large inlet VSD, dilated pulmonary annulus, large PDA. Small left ventricle with small aortic annulus and incompletely visualized aortic arch. Main pulmonary artery severely dilated. Color Doppler: Bidirectional shunting at the atrial level, Case of the week 08:10 – Interrupted Aortic Arch a b predominantly left to right. Flow across PDA also appeared bidirectional. CMR with contrast 3D MRA Aortogram: Real time cine images demonstrated complete interruption of aortic arch after LCCA (Type B). The dotted line in images a, and b shows where the course of the aorta should be. From the 3D angiogram LSCA arises post-ductal. Large PDA supplies entire descending aorta creating a “pseudo-arch appearance”. Perspective: CMR in conjunction with 3D MRA allows for diagnosis of interrupted aortic arch even in very young (< 48 hours life) pediatric patient without the risk of radiation. Cory Nitzel, Nishant Kalra, Dena Wilson, J Carlos Macias, Vincent Sorrell. Sarver Heart Center, University of Arizona, Tucson, Arizona,USA. Handling Editor: Mark Westwood