Download
1 / 35
350 likes | 384 Views
Learn about the most common cardiovascular disease, hypertension, its risks, causes, and treatment guidelines with a detailed case study analysis. Identify drug interactions based on symptoms, including sympatholytics, vasodilators, and renin-angiotensin system inhibitors.

E N D
Antihypertensive Drugs Fall ‘09 DIURETICS (only those used for antihypertensive therapy) SYMPATHOLYTICS Peripheral adrenergic receptor blockers Centrally acting RENIN-ANGIOTENSIN SYSTEM INHIBITORS Angiotensin Converting Enzyme (ACE) Inhibitors Angiotensin II receptor blockers VASODILATORS Ca2+ -channel blockers Others Treatment Guidelines from The Medical Letter Drugs for Hypertension January 2009
Hypertension • The most common cardiovascular disease • Affecting ~50 million people in the US • Defined as sustained systolic BP 140 mmHg and/or • Sustained diastolic BP 90 mmHG Causes: ~90-95% unknown origin (essential or primary hypertension) ~5-10% due to renal, endocrine or neurogenic disease
Risks associated with chronic elevated BP Stroke Heart Disease Heart Failure Arrhythmias Myocardial Infarcts Renal Failure
Strategies for treating hypertension • Stepped care approach: • Life style changes (e.g., lower dietary Na+, weight loss) • Single-drug therapy • Multiple-drug therapy Careful consideration should be taken when patients present with co-morbidities: diabetes, lipid disorders, ischemic heart disease and failure, migraines, asthma, etc... Specific patients may respond better to certain therapies (factors include; ethnicity, age, etc…)
JDM is an 81 year old caucasian male who has been active until the last 6 months. He lives in New England for 4 months of the year, and in the Bahamas for the remainder of the year. He exercises every day (typically a long walk), fishes and gardens. His longstanding PCP retired last year, and complains to his new PCP that he has bouts of light headedness and elevated heart rates. His wife is a retired nurse so she makes him take his blood pressure and heart rate often. Systolic pressure is usually normal, but diastolic pressure is low. AM Meds: Digitek (digoxin) 250 mcg Verapamil SR Tab, 180 mg Hydralazine 25mg Fish Oil 1000 units Enalapril Mal Tabs (5 mg in AM, 5mg in PM) ASA 350mg Chlorathalidone 25mg Multivitamin Ester C 1000 units/ MSM 1000 units Glucosamine/chondroitin/MSM 1000 units Acetaminophen 1000 mg (for arthritis discomfort) PM Meds: Terazosin (5 mg at noon, 5mg in PM) Hydralazine 25mg Lipitor 10mg Fish Oil 1000 units Flomax .4mg Singulair 10mg Acetaminophen 1000 mg (for arthritis discomfort) Glucosamine/chondroitin 1000 units/ MSM 1000 units For allergies/ asthma: Advair Discus 100/50, 1 one puff in AM, PM Fluticasone, 2 puffs each nostril once a day Maxair Autohailer, q4-6hr (rescue only) Claritin (generic) 10mg Can you identify potential interactions among the drugs based on sympotoms?
= = 4 SYMPATHOLYTICS VASODILATORS ANGIOTENSIN INHIBITORS Angiotensin Converting Enzyme (ACE) Inhibitors Angiotensin II receptor blockers Renin inhibitor DIURETICS 8 Brenner Fig 10-1
SYMPATHOLYTICS (see Table 9-1, Brenner) Peripheral adrenergic receptor blockers -blockers: propranolol, pindolol, metoprolol, atenolol -blockers: prazosin (1-blocker), phenoxybenzamine (1- and 2-blocker) 1-, 2- and 1- blockers: carvedilol, labetalol Centrally acting drugs clonidine (2-agonist) methyldopa (false transmitter) Ganglionic blockers: trimethaphan (rarely used in the US, if at all, only for hypertensive emergencies only)
Relative Receptor Affinities Alpha agonists Phenylephrine 1>2>>>> Clonidine 2 >1>>>> Mixed alpha and beta agonists Norepinephrine (NE) 1=2; 1>> 2 Epinephrine (Epi) 1=2; 1= 2 Beta agonist Dobutamine 1> 2 >>>> Dopamine agonist Dopamine D1=D2>> >> modified from Katzung Table 9-2
1 ADH Lippincott Fig 19-7
vasoconstriction (NE) vasodilation (Epi) Presynaptic inhibition of NE release blood glucose (from muscle and liver) bronchodilation + inotropic + chronotropic Not on same tissue NE Brenner Fig 8-1
See Drugs for angina and heart failure for details -Adrenergic Receptor Blockers Non-selective:1-, 2-blocker propranolol Selective: 1-blocker metoprolol, atenolol 1-, 2- and 1- blocker: carvedilol, labetalol both indicated for hypertension carvedilol also approved for heart failure patients Note: Nebivolol (approved 1/08) 1-blocker with antioxidant and increases endothelial nitric oxide release (vasodilator)
-blockers: Prazosin • Selective 1-blockers • TPR because of vasodilation • (not typically first line drugs) • No adverse metabolic or lipid effects • **therefore, advantage over –blockers with co-morbidities • Side effects: (Why might these be expected?) • Postural hypotension (especially after first dose) • Occasional reflex tachycardia – tries to compensate • Fluid retention Doxazosin significant increase in CHF compared to diuretics alone (ALLHAT) perhaps because of fluid retention
vascular 1 receptors Prazosin Intact feedback inhibition of NE release by 2 receptors 1 unless dose is too high Brenner Fig 9-4
= ? blockers = ? blockers TPR Before After CO Before After MAP Brenner Fig 9-3 Before After
Clonidine(2-agonist) For severe, refractory hypertension Side effects include: sedation, dry mouth, and rebound hypertension upon withdrawal after chronic use Centrally acting sympatholytics: TPR -Methyldopa(false neurotransmitter) Chronic therapy Replaces NE: Less effective for stimulating 1-receptors More effective for stimulating 2-receptors
*Clonidine X 2 * X -Methyldopa Brenner Fig 8-1
RENIN-ANGIOTENSIN SYSTEM INHIBITORS Angiotensin Converting Enzyme (ACE) Inhibitors: Captopril, Lisinopril (many on the market: enalapril, ramipril...) Angiotensin II receptor blockers (ARBs): Losartan (many on the market: candesartan, irbesartan, valsartan...) Direct renin inhibitor (DRI): Aliskiren Examples of indications and clinical uses: Mild/moderate essential hypertension Heart Failure (especially early stages) Diabetic nephropathy!!!!
PGs NO + H2O retention & vasoconstriction Na+ retention PGs = prostaglandins Brain Antidiuretic Hormone (ADH = vasopressin) (AT1) modified Brenner Fig 10-3
Captopril (prototype) • Highest oral bioavailability • Shortest t1/2 How would this affect dosing? • ACE-Inhibitors • Differ in their pharmacokinetics • Half-life (T1/2), metabolism • No adverse effects on lipid profiles or glycemic control • All have cardioprotection independent of BP • especially in CAD patients (HOPE Trials, NEJM 2000) • Also effective in reducing vascular complications • associated with diabetes (type 1 definitely, maybe type 2) • especially effective with nephropathies • (via anti-inflammatory mechanisms?) Less effective in blacks unless combined with thiazide diuretics (Medline 2003; Circulation 2005; 112:3654-3666)
Why? ACE-Inhibitors (con’t) Side effects related to: Suppression of angiotensin II (AngII) (hypotension and renal insufficiency) Increased in bradykinin (cough and edema) Also: Hyperkalemia (caution with K+ sparing diuretics) Fetotoxic (do not use with pregnancies) Renal failure (with bilateral renal a. stenosis) Bonus: Bradykinin stimulates vasodilation and Prostraglandin/NO vasodilation (high doses of NSAIDs may interfere with PGI2-mediated vasodilation)
Losartan Blocks AngII from binding to AT1 receptors Allows AT2 receptors to be stimulated by circulating AngII (promoting vasodilation????) Relatively few side effects less cough than with ACE-I but fetotoxic like ACE-I Diabetes: slows progression of nephropathy (RENNAAL) Cardioprotection (maybe??): reduces cardiac remodeling Typically reserved for patients who do not tolerate ACE-I Some evidence ACE2 metabolizes AngII to Ang1-7 (a vasodilator), and there are non-ACE sources of AngII, therefore ARB’s might be more effective than ACE-I (stay tuned, more data is needed) Less effective antihypertensive in blacks (same as with ACE-I)
Aliskiren: Direct renin inhibitor (DRI) New class of nonpeptide, oral inhibitor Binds to a site on renin, preventing formation of angiotensin (Ang) I Lowers plasma renin activity, Ang I, Ang II, and aldosterone Safety and tolerance appear similar to ACE-I and ARBs • Significance of inhibiting renin? • ACE-I and ARBs may increase renin • (because no negative feedback) • Hydrochlorothiazides also increase renin • Pro(renin) receptors were recently identified • Activate MAP kinases and profibrotic signaling • May be involved in vascular remodeling (e.g., with diabetes)
VASODILATORS Ca2+ -channel blockers: DHPs: amlodipine, nifedipine Diltiazem Verapamil Others: less frequently used for chronic Tx Hydralazine Minoxidil Note: nitrates not used for chronic hypertensionTx sodium nitroprusside (SNP): used for hypertensive emergencies and surgery) (cyanide toxicity due to metabolite – obsolete story)
Why would this be an advantage over other drugs such as -blockers? • VASODILATORS (con’t) • Promote vascular smooth muscle relaxation, TPR • Most (not all) produce concomitant reflexes if not dosed properly: • cardiac contractility and HR • myocardial O2 consumption • renin-angiotensin-aldosterone system • Usually no effects on serum lipids
Ca2+ channel blockers (CCBs) • Site of action dependent on tissue selectivity • Verapamil • most cardiac selective (nodal cells and myocytes) • Diltiazem • intermediate selectivity • Dihydropyridines (DHPs) • most vascular selective All have some coronary vasodilatory effects Which is most likely used for antihypertensive therapy? Which is most likely to cause reflex tachycardia? See also Angina drug & Antiarrhythmic drug lectures
Why? Toxicities associated with DHPs (selected) Short acting DHPs Immediate-release nifedipine, nisoldipine, felodipine May cause reflex tachycardia Longer acting DHPs Sustained-release nifedipine, amlodipine, isradipine Do not cause significant increases in HR (neither do verapamil or diltiazem) • Side effects of DHPs include: • Headaches • Peripheral edema Doses to achieve BP goals will likely differ from anti-anginal goals, therefore side effects may be different
Hydralazine and Minoxidil • Typically reserved for severe hypertension • Often co-administered with a diuretic and/or -blocker • Dilates arterioles, not veins • contraindicated for patients with angina, ischemic heart disease • Hydralazine • May act by increasing cGMP (similar to NO) • (in combination with isosorbide dinitrate – see HF lecture) • Minoxidil (oral, not topical) • Opens KATP channels, thus hyperpolarizes cells
Ca2+ contraction MLCK PDE PDE GMP cGMP cAMP AMP K+ATP Vascular Smooth Muscle Cell sites of antihypertensive drug action Sildenafil cGMP PDE5 inhibitor (not used for systemic hypertension, but maybe pulmonary arterial hypertension) CCB DHP A1 Blocker Prazosin ACEI Renin inhibitor ARB Losartan blocker agonist Ca2+ NE Minoxidil AII 1 AT1 SR Ca2+ b2 Hydralazine Epi NO Endothelial cell Acetylcholine Bradykinin PDE = phosphodiesterase
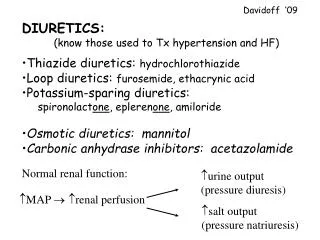
DIURETICS: • (those used for antihypertensive therapy) • Thiazide diuretics: • hydrochlorothiazide • Loop diuretics: • furosemide • Potassium-sparing diuretics: • amiloride, spironolactone, eplerenone Discussed previously
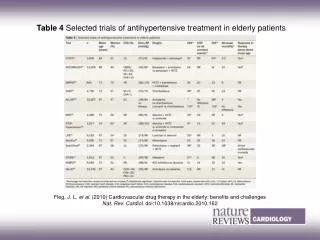
Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) Arch Int Med 2008, 168(2) update Thiazides are DOC in hypertensive patients with metabolic syndrome No evidence that ACEI, CCB, alpha blockers offer any advantage of clinical outcomes over thiazides in these patients (particularly in blacks with metabolic syndrome) chlorthalidone, lisinopril, amlodipine, doxazosin Doxazosin arm stopped early because of increased CV events, with 2x more HF compared to thiazide group
JNC VII Compelling Indications for Drug Classes Compelling Indication Initial Therapy Options Clinical-Trial Basis Heart Failure Diuretic, BB, ACEI,ARB, Aldo Ant MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, Val-HeFT, RALES Post-MI BB, ACEI, Aldo Ant ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS High CAD Risk Diuretic, BB, ACEI, CCB ALLHAT, HOPE, ANBP2,LIFE, CONVINCE Diabetes Mellitus ACEI, Diuretic, BB, ARB, CCB NKF-ADA Guideline,UKPDS, ALLHAT NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK Chronic Kidney Disease ACEI, ARB Recurrent Stroke Prevention Diuretic, ACEI PROGRESS ACEI=Angiotensin converting enzyme inhibitor, Aldo Ant=Aldosterone antagonist, ARB=Angiotensin receptor blocker, BB=b-blocker, CAD=Coronary artery disease, CCB=Calcium channel blocker, MI=Myocardial Infarction Chobanian AV et al. JAMA. 2003;289:2560-2572
Clinical considerations: Most effective treatment, ethnicity differences* Least side effects (most patients are asymptomatic) Frequency of dosing Cost Fixed-drug combinations: -blocker and thiazide diuretic ACE inhibitor and thiazide diuretic AII receptor blocker and diuretic Ca2+ channel blocker and ACE inhibitor What are advantages and disadvantages of fixed-drug combinations?
Presence of co-morbidities (considerations) • Thiazide diuretics and -blockers: • Often used in combination • However, both may adversely affect lipid profiles and insulin sensitivity (exaccerbate CAD, atherosclerosis, type 2 diabetes) • ACE inhibitors: • May also be beneficial for diabetic nephropathies • ACE inhibitors and diuretics: • Useful for patients with CHF • -blockers or Ca2+ channel blockers: • Useful for patients with angina • Diuretics and Ca2+ channel blockers: • Blacks respond better to each, rather than to -blockers and ACE inhibitors
Antihypertensive Targets (-) ARBs = angiotensin receptor blockers; AT-1 = angiotensin II sub-type 1; DHPs = dihydropyridines; SVR = systemic vascular resistance. (LH Opie, 2004.)
Guidelines for treatment and prevention of hypertension are published by the Joint National Committee (JNC) on the Detection, Prevention and Treatment of Hypertension Guidelines and updates (including power point presentations, treatment algorhythms, etc…) can be found (free) through the NHLBI website http://www.nhlbi.nih.gov/guidelines/hypertension/ http://www.nhlbi.nih.gov/guidelines/hypertension/ http://www.nhlbi.nih.gov/health/prof/heart/index.htm#hbp http://www.nhlbi.nih.gov/health/prof/heart/index.htm#hbp