Download
1 / 24
910 likes | 5.64k Views
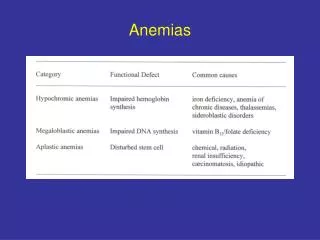
Sideroblastic Anemias. Microcytic, hypochromic anemias. Fe-deficiency Anemia of chronic diseases Sideroblastic anemias, esp. lead poisoning Thalassemias. Hemoglobin (HEME+GLOBIN).

E N D
Microcytic, hypochromic anemias • Fe-deficiency • Anemia of chronic diseases • Sideroblastic anemias, esp. lead poisoning • Thalassemias
Hemoglobin (HEME+GLOBIN) • Adult human bone marrow synthesizes 4X1014 molecules of hemoglobin every second. Hemeand globin chains (alpha and beta) in adults are manufactured in separate cell compartments, mitochondria and cytoplasm, respectively, and then combined in cytoplasm in an amazingly accurate manner.
Four major problems can manifest during this delicate process: • •Qualitative defects of globin chain synthesis result in hemoglobinopathies such as sickle cell disease. • •Quantitative defects of globin chain synthesis result in hemoglobinopathies such as thalassemia. • •Defects in synthesis of the hemeportion result in porphyrias. • •Defects involving incorporation of iron into the heme molecule result in sideroblasticanemias.
Ala-dehydrogenase δ ALA-synthase PBG-deaminase Uro’gen III synthase Ferrochelatase Proto’gen III oxidase Uro’gen III decarboxylase Copro’gen III oxidase Heme synthesis Cytoplasm Mitochondrion Succinyl-CoA + 5-amino levulinic acid porphobilinogen Glycine hydroxymethylbilane Heme uroporphyrinogen III Protoporphyrin IX coproporphyrinogen III Protoporphyrinogen III
Overview of Iron and Heme ha11g09
Overview of Heme synthesis ha47g04
SideroblasticAnemias Sideroblastic anemias, a group of heterogenous disorders, produce a common defect—failure to use iron in hemoglobin (Hb) synthesis, despite the availability of adequate iron stores.
Sideroblastic Anemias This is a refractory anaemia with hypochromic cells in the peripheral blood and increased marrow iron; It is defined by the presence of many pathological ring sideroblasts in the bone marrow
SideroblasticAnemias • Disease that interfere with production of heme • May be microcytic and hypochromic • Iron abundant in marrow (in contrast to IDA) • Prussian stain shows normoblasts with iron deposits in mitochondria surrounding nucleus • Ringed sideroblasts are hallmark
Stainable bone marrow iron • Iron – stored in reticuloendothelial cells • Iron granules – formed in normoblasts • Ferritin = iron + apoferritin protein • Hemosiderin = iron-protein complexes with high iron content, and denature ferritin aggregates • Hemosiderin in reticuloendothelial cells, every 3rd - 4th oil immersion field • Sideroblast = nucleated RBCs with iron granules • Siderocyte= anucleate RBC with iron granules • Ringed sideroblast= 5+ distinct granules, at least 1/2 of perimeter
Example of ringed sideroblasts http://www.som.tulane.edu/classware/pathology/Krause/Anemias/Sid_RS.HTML
Eitology of Sideroblasticanemias • Hereditary • X-linked (isolated / genetic syndromes) • Autosomal • Acquired • Drugs (chloramphenicol, isoniazid) • Heavy metals (e.g. lead) • Chemotherapeutic agents • Clonal (RARS, RARS-T, RCMD-RS)
Signs and symptoms • nonspecific clinical effects, which may exist for several years before being identified. Such effects include • anorexia, • fatigue, • weakness, • dizziness, • pale skin and • mucous membranes and, occasionally, • enlarged lymph nodes. • Heart and liver failure may develop from excessive iron accumulation in these organs, causing dyspnea, exertional angina, slight jaundice, and hepatosplenomegaly. • Hereditary sideroblastic anemia is associated with increased GI absorption of iron, causing signs of hemosiderosis. Additional symptoms in secondary sideroblastic anemia depend on the underlying cause.
Diagnosis • CBC: Microscopic examination of blood shows hypochromic or normochromic, and slightly macrocytic, erythrocytes. • Bone Marrow: Ringed sideroblasts on microscopic examination of bone marrow aspirate, stained with Prussian blue or alizarin red dye, confirm the diagnosis. • Red blood cell (RBC) precursors may be megaloblastic, with anisocytosis (abnormal variation in RBC size) and poikilocytosis (abnormal variation in RBC shape). • Unlike iron deficiency anemia, sideroblastic anemia lowers Hb and raises serum iron and transferrin levels. In turn, faulty Hb production raises urobilinogen and bilirubin levels. Platelet and leukocyte levels remain normal, but thrombocytopenia or leukopenia occasionally occurs.
Treatment • The underlying cause determines the type of treatment. • Hereditary form • Hereditary sideroblastic anemia usually responds to several weeks of treatment with high doses of pyridoxine (vitamin B6). • Primary acquired form • Elderly patients with sideroblastic anemia—most commonly the primary acquired form—are less likely to improve quickly and are more likely to develop serious complications. Deferoxamine may be used to treat chronic iron overload in selected patients. • Carefully cross-matched transfusions (providing needed Hb) or high doses of androgens are effective palliative measures for some patients with the primary acquired form of sideroblastic anemia. However, this form is essentially refractory to treatment and usually leads to death from acute leukemia or from respiratory or cardiac complications. • Secondary acquired form • The secondary acquired form generally subsides after the causative drug or toxin is removed or the underlying condition is adequately treated. Folic acid supplements may also be beneficial when concomitant megaloblastic nuclear changes in RBC precursors are present.
Lead poisoning • Interferes with porphyrin synthesis at two steps: • Conversion of aminolevulinic acid to porphobilinogen… • Aminolevulinic acid accumulation • Incorporation of iron into protoporphyrin IX by ferrochelatase • Iron and protoporphyrin accumulation • More significant inhibition of two steps • Measure in urine accumulated aminolevulinic acid • Measure in RBC extract as FEP or zinc protoporphyrin
Ala-dehydrogenase ALA-synthase PBG-deaminase Uro’gen III synthase Ferrochelatase Proto’gen III oxidase Uro’gen III decarboxylase Copro’gen III oxidase Figure 19-5: Heme synthesis Mitochondrion Cytoplasm Succinyl-CoA + 5-amino levulinic acid porphobilinogen Glycine Lead hydroxymethylbilane Heme uroporphyrinogen III Protoporphyrin IX coproporphyrinogen III Protoporphyrinogen III
Anemia in context of lead poisoning • Normocytic and normochromic • Chronic exposure may lead to microcytic, hypochromic anemia • Also results in hypoplasia of bone marrow • Basophilic stippling seen • Reticulocyte count can be elevated • Due to hemolytic component • Can be seen by impairment of pentose-phosphate shunt by lead, leading to oxidant-sensitive stress
Summary of sideroblastic anemias • SA develops when entry of iron into mitochondria of developing RBCs is blocked • Iron incorporation into heme blocked by any deficiency of enzymes of heme synthetic pathway • Iron accumulates in mitochondria in deposits around nucleus, called ringed sideroblasts • Iron studies – elevated total iron, variable iron binding capacity, normal to decreased transferrin saturation, and increased ferritin